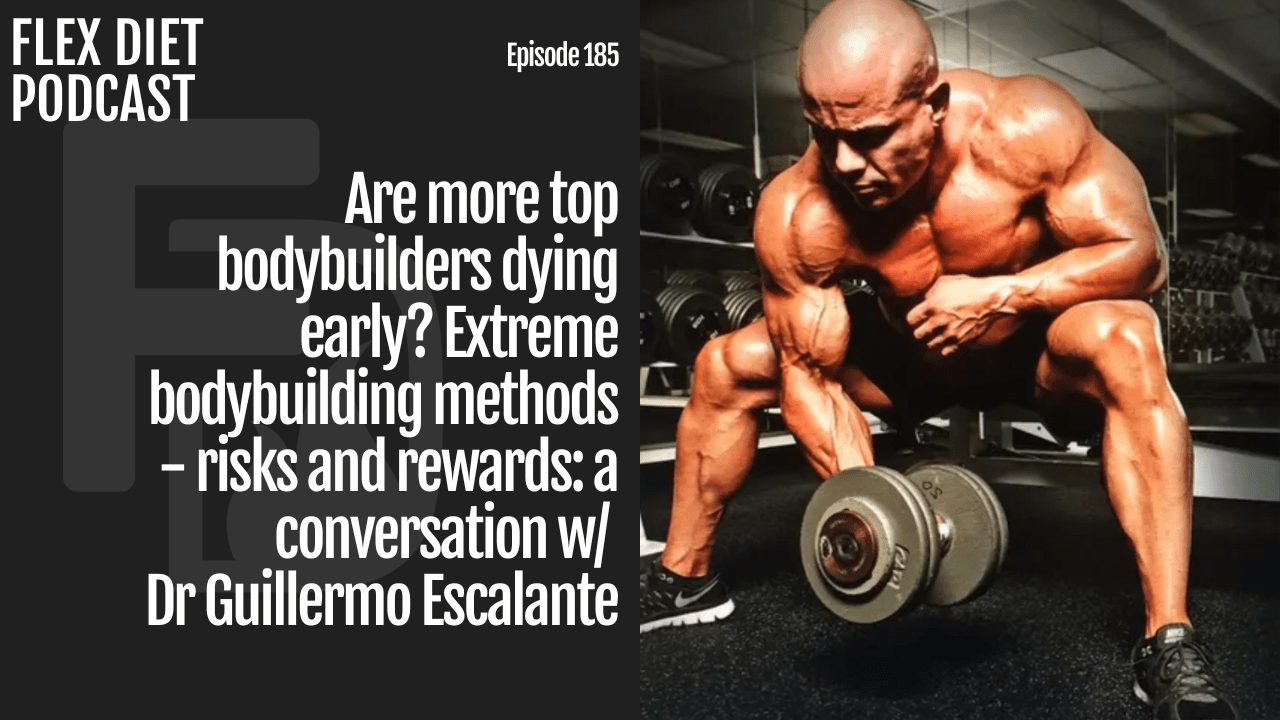



Are more professional bodybuilders dying early, and, if so, why? Dr. Guillermo Escalante and I attempt to answer this question as we tackle the pros and cons of professional bodybuilding on today’s episode of the Flex Diet Podcast.
Dr. Escalante has competed at a high level in professional bodybuilding and has published extensively on the topic. He’s also a professor at California State University, San Bernardino.
Today’s episode is brought to you by miketnelson.com. Sign up for my fitness insider newsletter for daily training, nutrition, and sports performance tips.
Listen to hear:
- [6:10] Ways bros are ahead of physique science and ways they are behind
- [12:46] What people don’t know about pharmacology
- [15:46] Diuretics and risk
- [26:20] Has diuretic use increased?
- [34:43] The push toward extremism and the subjectivity of judging
- [42:49] Having the foundation matters
- [51:26] Bodybuilders who died young and risk factors
- [1:06:49] Cardiovascular training
- [1:11:23] Dr. Escalante’s advice
Connect with Dr. Escalante:
Referenced Links:
- Dead Bodybuilders Speaking from the Heart: An Analysis of Autopsy Reports of Bodybuilders That Died Prematurely
- Analysis of the efficacy, safety, and cost of alternative forms of creatine available for purchase on Amazon.com: are label claims supported by science?
- Can Bodybuilding Peak Week Manipulations Favorably Affect Muscle Size, Subcutaneous Thickness, and Related Body Composition Variables? A Case Study
- Flex Diet Podcast Episode 107: Peak Week: How to Look Leaner by Manipulating Water, Carbs, Salt, and More with Dr Guillermo Escalante – Dr. Mike T Nelson
About Dr. Escalante:
From Dr. Escalante’s website
Dr. Escalante is currently a Professor of Kinesiology and Dean Fellow for the College of Natural Sciences at California State University, San Bernardino. He is a scholar in the areas of exercise science, sports nutrition, and sports medicine. His research interests include sports nutrition/supplementation, body composition assessment, physique enhancement, and sports injury prevention/rehabilitation. Dr. Escalante has over 52 peer-reviewed publications and abstracts in the fields of exercise science, sports nutrition, sports medicine, and kinesiology. He regularly presents at regional, national, and international conferences on his research and serves as a sports nutrition/exercise science consultant to various companies in the health/fitness/sports supplement space. Additionally, he has served as an expert witness in the areas of sports nutrition and sports medicine. Dr. Escalante has secured over $150,000 of internal funding to support his teaching and research as well as over $5 million in external funding as principal investigator or co-investigator through various businesses and agencies, inclusive of the US Department of Education and the US Department of Veteran Affairs.
Dr. Escalante holds a BS in Athletic Training with a Biology minor and an MBA with concentrations in Marketing and Healthcare Management from the University of La Verne. He also received a Doctor of Science in Athletic Training from Rocky Mountain University of Health Professions and is certified as an athletic trainer through the National Athletic Trainer’s Association (NATA), a strength and conditioning specialist through the National Strength and Conditioning Association (NSCA), and as a Sports Nutritionist through the International Society of Sports Nutrition (ISSN). In 2021, Dr. Escalante became one of only 36 fellows (out 36,000+ members) of the ISSN for his contributions in the field of sport nutrition. Dr. Escalante is an active member of the NATA, NSCA, and the ISSN. He serves as a reviewer and associate editor for the Journal of the International Society of Sports Nutrition (JISSN), is the chair of the NSCA Bodybuilding and Fitness Special Interest Group, and is on the executive board for the NSCA Nutrition and Metabolism Special Interest Group. He also serves as a reviewer for 8 major journals including the Journal of Strength and Conditioning Research and the British Journal of Nutrition.
Dr. Escalante also has over 50 publications in mainstream fitness magazines and websites including Muscle & Fitness, Muscle & Fitness Hers, Bodybuilding.com, Muscular Development, and MuscleMag International Magazine. He has appeared on television, radio shows, and podcasts discussing fitness, health, bodybuilding, and performance enhancement drugs. He has been a competitive bodybuilder since 2000, a bodybuilding/physique coach since 2004, and was a bodybuilding judge and/or sports medicine provider for MuscleContest International from 2010-2019.
Dr. Escalante is an instructor with the Kaiser Permanente Post-Doctoral Physical Therapy Orthopedic and Sports Fellowship programs where he teaches post-doctoral physical therapy fellows sports nutrition and practical applications of exercise science for sports performance enhancement. He was also an instructor to third year Doctor of Physical Therapy students at Western University of Health Professions between 2004-2018.
Prior to going into higher level education, Dr. Escalante owned and operated an outpatient orthopedic physical therapy and personal training business for 18 years and was an owner/operator of 2 World Gym franchises. He also served as interim head athletic trainer for East Los Angeles Community College, was a fitness/health consultant for the US Department of Defense, and was the Chief Operating Officer and Sports Medicine Coordinator for a large physical therapy/sports medicine practice in Southern California. Over the course of his 20+ year career, Dr. Escalante has had the opportunity to train, treat, coach, and/or consult with thousands of athletes and non-athletes alike inclusive of professional athletes in the NFL, MLB, NBA, LPGA, Olympians, and IFBB bodybuilders/physique competitors.
Dr. Escalante prides himself in his commitment to life-long learning and professional development. When he is not reading, researching, writing, or teaching, you can find him in the gym working out, walking his dogs, in the kitchen making delicious nutritious food, riding his Harley, and enjoying time with his wife and family traveling or watching TV at home. Dr. Escalante also enjoys singing under his alter-ego “Gil” and is working on his skills in stand-up comedy.
Rock on!

Dr. Mike T Nelson
Download the transcript

Full text below

Dr. Mike T Nelson
PhD, MSME, CISSN, CSCS Carrick Institute Adjunct Professor Dr. Mike T. Nelson has spent 18 years of his life learning how the human body works, specifically focusing on how to properly condition it to burn fat and become stronger, more flexible, and healthier. He’s has a PhD in Exercise Physiology, a BA in Natural Science, and an MS in Biomechanics. He’s an adjunct professor and a member of the American College of Sports Medicine. He’s been called in to share his techniques with top government agencies. The techniques he’s developed and the results Mike gets for his clients have been featured in international magazines, in scientific publications, and on websites across the globe.
- PhD in Exercise Physiology
- BA in Natural Science
- MS in Biomechanics
- Adjunct Professor in Human
- Performance for Carrick Institute for Functional Neurology
- Adjunct Professor and Member of American College of Sports Medicine
- Instructor at Broadview University
- Professional Nutritional
- Member of the American Society for Nutrition
- Professional Sports Nutrition
- Member of the International Society for Sports Nutrition
- Professional NSCA Member
[00:00:00] Dr Mike T Nelson: Welcome back to the Flex Diet podcast. I’m your host, Dr. Mike T. Nelson. And on this podcast, we talk all about. Things to help you with better body composition performance. All in a flexible based approach in a wide variety of other topics also. Today on the podcast. We have my good buddy, Dr. Guillermo Escalante and we’re talking all about.
Professional bodybuilders. And physique athletes. What are some of the pros and cons? And why does it appear? A fair amount of them have been passing away. Unfortunately, at very young ages. Is this related to. Health parameters, pushing performance too hard. Diuretics other types of drugs and maybe even cardiovascular health.
So we dig into all of that. Today. Dr. Escalante. Has competed both in professional bodybuilding at a very high level. Is a professor out in California. And has published extensively on this topic. So he’s got the trifecta of knowledge to help us sort through all of the fact versus fiction in this area.
And again, it goes without saying. None of this is medical advice. We were just talking to him about the current published research. At the end of the day. Everyone has to track and decide for themselves. What they feel best. And if you’re listening to this in the U S. Many of the drugs we talk about.
Especially performance enhancing drugs. Are still considered illegal at the federal level. So not only are there potentially. Ethical considerations. There are legal considerations also. None of this is necessarily advice or just want to have an educated discussion about. What does the research say?
And the goal is to provide more awareness to people. If you enjoy this podcast. Check out more information from yours. Nerdy here. Go to miketnelson.com. That is the main website that everything goes through. You can hop onto the newsletter there via various methods. And send me a note saying that you listened to the podcast.
And I’ll send you a free gift. I promise there’ll be something cool. So go to Mike T nelson.com. Get on the newsletter. Send me a note there. And even if it’s just a say hi, give me some feedback. Do you like the podcast? Who do you want to see? Same thing with the daily newsletter. So as of now, I’m the only person that sponsors this podcast. So I get to do.
Whatever the heck I want. And talk to whoever I think is interesting, who has. Great information to pass along to you. So enjoy this interview with Dr. Escalante.
[00:03:25] Dr Mike T Nelson: Welcome back to the Flex Diet Podcast, and I’m here back with a guest once again. Dr. Escalante, how are you doing today, sir?
[00:03:35] Dr. Guillermo Escalante: Doing great. Today, Dr. Nelson. Thank you for inviting me. I appreciate you having me on the podcast again. It was fun last time, and I’m sure it’ll be no different
[00:03:42] Dr Mike T Nelson: this time. Yeah.
Yeah. So we’ll link to the episode. Last time, eh, some of this might overlap a little bit, but today you just published, this was a couple of weeks ago now, some super interesting data on some autopsies from professional bodybuilders. And I’m sure we’ll link to the articles in the Washington Post.
And I, I think there was a subset of an msn just talking to him about the risks with everything from fitness competitions, physique body building. And so since you’ve actually competed at a very high level in the sport, and you’ve actually written on the topic, we wanted to get you back on here since you would be the perfect person to discuss this in more
[00:04:21] Dr. Guillermo Escalante: detail.
Yeah, I appreciate it. Yeah, it’s been it’s been nice. We’ve really gotten a lot of good information out of there. And I think. One of my missions over the last few years really has been to try to make body building and fitness just a, a sport that I’ve obviously loved for the last 24 years, just to make it safer for the individuals that are practicing it and and obviously a little bit more evidence-based as much as possible.
Tho you know, along those two lines it’s been nice to be able to try to begin to play a role in that, but there’s still a steep hill to climb and I think this is a good beginning to getting
[00:04:51] Dr Mike T Nelson: on that road. So you’re saying, you mean there’s actually like bro science and other people who are scientists in the body building field
[00:05:00] Dr. Guillermo Escalante: Yeah. Yeah. Imagine that. Yeah. There there’s a lot of bro science and I always say not to knock all the bro science because, as you and I know sometimes bros actually have it right a lot of the time. A hundred percent. Yeah. And it’s a matter of, discerning the myths from the rest of it and and then figuring it out.
And really my mission has been what the NSA’s mission is just to bridge the gap between science and application specifically in this physique field because there’s just so much misinformation out there and there’s a lot of stuff that is, you know bogus.
But there’s also a lot of good information that is available that has been done for many years where, you know, some of the bro practitioners have been doing it for, decades and scientists are just now studying and applying the scientific method behind all of it and really seeing, okay, yeah, this there’s definitely some merit to some of these things and we can tweak some of these things.
And then, yeah, some of this stuff we can throw it in the trash bin because it’s really not relevant. I’ve really enjoyed playing a part in putting those pieces of the puzzle
[00:05:54] Dr Mike T Nelson: together. Yeah. This is a two part question, but, so part one would be, what were some things, do you think that the bros were actually way ahead of the science, and then the flip of that, where do you think the science is ahead of some of the bro.
[00:06:10] Dr. Guillermo Escalante: Yeah. I think some of the basic stuff I would say, like high protein intake, that they’ve been doing that for decades. I don’t know, for 40, 50, 60 years, I think bodybuilders have been consuming probably pretty close to about a gram per pound of body weight of protein, for many years.
And of course the medical community, and even some today will still say, oh, don’t take more than the R d a or too much more than the R D A and and I think there’s definitely too much protein at one end, at some point. But we, we do have to find that sweet spot where they are.
And I think. About 2.2 grams per kilogram. That kind of seems to be a pretty good, sweet spot for most physique competitors, maybe on a hyper caloric diet, maybe going slightly higher than that. So that’s one that stands out to me. I think obviously, training volume as it relates to muscle hypertrophy, that’s something that, that bodybuilders have been doing for a long time is training with adequate volume and intensity for that matter in, in regards to their training programs.
I also think some of the other components in terms of just that are not necessarily in, in the good side of things would be, how extreme do you have to be? So before it’s you think of even when I started body building, it’s our typical diet was.
Hey you need to quote unquote eat clean and you can only eat, broccoli and chicken breasts, and your next meal should be broccoli and chicken breasts. And then of course, the thin the skin you then need to eat. Tilapia only.
[00:07:27] Dr Mike T Nelson: Tilapia. Only tilapia does that. , nothing else.
Milk. Oh my god, your skin would be so thick. You’re screwed. .
[00:07:34] Dr. Guillermo Escalante: So tho those are some of the myths that we actually, you know actually see. And it’s okay, yeah, that, that’s, we can throw that by the wayside. And then I think there’s a lot of stuff that we’re still finding out, in terms of and we need to dive deeper into the science.
And then of course, there’s this stuff that we really can’t study because of medical ethics and IRBs and all of that. We’re never gonna really be able to do randomized control trials with, what’s the ideal drug intake that’s used for performance enhancement? Performance enhancement purposes.
That’s never gonna happen. We’re never gonna have evidence-based ways to do this. All we all we can do is what’s being done and study what’s being done, and then hopefully being able to decipher, good safety measures into what are better ways, more conservative ways, and what can we be looking for so that we are not putting yourself at extreme risk of any, anytime you’re doing anything to an extreme level, there are risk involved, but how can we mitigate those risks and at least be aware of what we’re stepping into.
[00:08:30] Dr Mike T Nelson: Yeah. And do you think there’s times where the science is ahead of what some of the bros are doing now? Because I know that the, I won’t name any coaches, but certain coaches have been famous for saying, what we’re doing is like 10 to 15 years ahead of the science and then in some ways that’s true.
But any thoughts on where science might be ahead or at least is hinting towards things that is not necessarily popularly done for body building in terms of training or
[00:08:59] Dr. Guillermo Escalante: nutrition. Yeah, I would say one that kind of stands to mind I was actually talking to Eric Hels about this just a couple
[00:09:06] Dr Mike T Nelson: days ago.
[00:09:06] Dr. Guillermo Escalante: Oh, nice. Today. Yeah. And we were talking the water manipulation part, right? I think there’s still a lot of ambiguity there on, is it really necessary to deplete water before, before a competition? And I’m not a big advocate of eliminating water ever but maybe titrating down a little bit, but never eliminating but still keeping, a constant flow and being very specific with the timing.
Or maybe even is that even really necessary? Can we actually just maintain that? Cuz and this comes a lot with the terminology of what’s used in the industry, where they say, Hey, you need to come in a little drier. You need to look, you need to, he’s so dry. He came imperfect.
He’s so dry. So that verbiage. Automatically associates to you to drinking less water. Or being dehydrated. And really, w what they probably really mean is they were really lean and being really lean actually creates a quote unquote dry look because there’s obviously less of a layer between the muscle and the and the skin.
Because that subcutaneous layer is now, minimal and of course you’re gonna be able to see more striations. So looking at that practice in particular, I think we’re starting to investigate it. We did a case report with Chris Baratt last year. I actually collected some data on myself for my.
My recent show in some Oh, nice. The practices. But there’s a lot of limitations in the methodology of what we’re doing to really identify it. Some of the next things we’re gonna look at is maybe looking at bio and penis spectroscopy with some base angle stuff to see if we can actually look at the raw data rather than the actual number that, that the b i s actually spits out.
Because that might be a little bit more telling. Cuz obviously when you’re, if you’re dehydrated, you’re automatically. , all of the principles that the machine thinks that you’re right, you’re in a dehydrated state. We’re not in a dehydrated state for depleting water. It, it may actually not be a a reliable number that you’re seeing when it’s says total body water or intracellular or extracellular water.
I think in that regard, I think the science may be a little bit of a head with some of that. Also things like a lot of bodybuilders maybe would carb. Carb load and sodium deplete at the same time. When it’s yeah, we need some sodium, depending, glucose strand, porters, we need sodium plays a role in your ability to carb load properly or maybe not drinking any water with the carb, bloating that, that could have some limitations as well.
So I think this is now where science has brought some light into this. It’s okay, now there is some benefit to drinking, adequate amounts of water while you’re car bloating. And there’s also some benefit to having an adequate sodium intake and electrolyte intake in general while you’re car bloating, so that you can actually absorb those carbohydrates.
So I think some of those practices, the science has actually shed a little bit of light and, it’s basic nutrition, nutritional biochemistry and metabolism when you actually see how these things are absorbed and metabolized. But applying some of those principles and studying them a little bit further has stuff I think has
[00:11:58] Dr Mike T Nelson: helped.
Yeah, and we talked a little bit about that with you on the last podcast. And then I did a podcast with a friend Michelle, welcome, where I talked about that too. And yeah, those two areas, it just feels like to me, maybe not so much with the last few years with natural competitors, but at least with enhanced competitors, it just seems like they just threw all the physiology textbooks out the window for , some odd reason.
And do you think part of that is possibly the use of diuretics? Because diuretic use will change that equation so drastically, where if you’re a natural competitor, you’re obviously not, hopefully not using any diuretics and that is just this big kind of sledgehammer that’s overriding some of the physiology is why those areas seem to be less appreciated.
[00:12:46] Dr. Guillermo Escalante: Yeah, I think that, that’s definitely a contributing factor. They they rely a lot on the pharmacology as needed. And unfortunately, they understand. And I’m not gonna say ever, there are some bright coaches that I’ve talked to that are very Oh, sure. But for the vast majority of them, really you’re really looking at individuals who have a cliff note version understanding of of how these drugs work and pharmacokinetics, pharmacodynamics of those drugs.
And at the end of the day even if you studied, chemistry and biochemistry in, in college at a decent level you’re still not a pharmacist. You’re not a pharmacologist, you’re not a physician. So you really have very limited knowledge.
And of course you can self-educate. And this is where I see, I do see some coaches that actually have, read the, the medical literature and they do understand some of these, and you can speak to them at a very high level. And to be honest, some of you even educated me in how I do, I don’t claim to know everything.
I like to always read and talk to people and understand things from everybody. But. That’s not the majority of the individuals that are out there. Unfortunately, a lot of the coaches that are out there maybe have had, success at the local level, maybe success at the national level, have done a handful of shows or maybe won a couple of shows themselves.
Maybe they’re naturally gifted themselves and then, they read the Cliff note version or the Instagram post version of it and or watch the YouTube version of it from unreliable sources. And then now they’re cookie cutting and prescribing. And I think that’s where you see these limitations.
And they know the right words to make them sound like they know everything. Yeah. But realistically, when you really try to have them explain everything in detail, they’re really missing a lot of big chunks that are very important to understand.
[00:14:25] Dr Mike T Nelson: Yeah. What I commonly see, The use of a few key terms with that doesn’t mean that they understand it.
They’re like, oh, this is a loop diuretic. And you’re like, oh, a loop di oh my God, you must know what’s going on. It’s you could have got that from Wikipedia. That doesn’t mean you know shit, . Exactly. Maybe you had some other people, sadly, but yeah, there is no guarantee that you’re gonna get it correct,
[00:14:45] Dr. Guillermo Escalante: per se.
Yeah, exactly. Exactly. Or they understand the sodium potassium pump. Okay so what, yeah. , that’s a very small part of some of this stuff, or or it’s a potassium sparing diuretic, okay, but so what does that mean in the big picture of things?
[00:15:01] Dr Mike T Nelson: Would you agree that in terms of if we’re looking at risk, That the acute risk in terms of the short term risk, that diuretics would probably be one of the more riskier things that enhanced competitors play
[00:15:14] Dr. Guillermo Escalante: with. Yeah, absolutely. And I think they’ve been almost glorified. Actually if you read some of the, some of the original textbooks on peds, the anabolic series, I don’t know what volume it’s up to.
I think I’m looking here on my shelf. I think I have. 11th edition here on there. But anyway even reading back from the very first edition or years ago, no, 20 some years ago you read diuretics are the secret to being shredded and to having that stage physique.
And that’s really not necessarily the truth. I I, not that they weren’t used, and did play a role. But that’s not, there’s a lot of danger to that. And you’re playing Russian roulette and Absolutely. I see. That’s probably the biggest contributor to to death actually.
They even anabolic steroids, they’re, you can take 400 milligrams of an anabolic on your arm or your thigh or butt, and and you’re not gonna die tomorrow. It’s a slow cumulative effect of the effects that it’s gonna have, and it affects people differently.
Not always the same way and in different dosages, but these diuretics, if you misdose them, and then you combine a lot of these things together. And when I see combined, it’s usually a combination of, yeah, I haven’t drank water for the last, two days, and I I’ve been taking these other, performance enhancement drugs that are maybe gonna be hard on the heart.
Maybe ephedra maybe clenbuterol maybe caffeine, stacking all those regularly. And then now on top of that, you’ve added this loop diuretic on top of that now you’re potentially putting your life at risk. And that, and they’re not understanding, that it’s one, one on its own is very powerful.
You combine these and that’s when you can potentially run into life-threatening problems. So for me, I think the first line of defense in terms of what can we do to. For the health and safety of athletes is basically educate people on extreme bodybuilding practices. And the number one that comes to mind is dropping water.
And, and what’s h how much water can you safely drop if you need to drop anything at all? And number two is, using these other external drugs that are prescription drugs to help facilitate that. I think that would be be the first point. If in fact if they’ve been, if they’ve had only one drug in the I F P B and the N P C.
I would vote test for diuretics. And I, and they did try to do that in the 1990s and it
[00:17:36] Dr Mike T Nelson: failed. Yeah. They did it for one year, I think, if I remember
[00:17:38] Dr. Guillermo Escalante: correctly. Yeah. And it, it didn’t work. But to me, I think that would be, that would solve a lot of the problems right off the bat is just to ban those or test for those even if it’s randomly so competitors know that Hey I can get disqualified for this.
And number two, provide education that’s not even necessary to take those measures.
[00:17:59] Dr Mike T Nelson: Yeah. I remember the first time I ever was, aware of it, I, you probably know what year it was the. The year they carried Paul, the lead off stage. It was just like, basically just completely frozen, like on death’s doorstep.
And I was like, what the hell? And at first, you’re thinking no drugs, and then you realize that, oh, they goofed up the diuretics and it’s oh man, that’s, oh, bad .
[00:18:21] Dr. Guillermo Escalante: Yeah. Yeah. Ronnie Coleman tells a story where he, he almost didn’t make it on stage. Yeah. He almost passed out from and there’s a lot of stories like that from a lot of different individuals that, that have done that.
And that was when I was working as an athletic trainer covering the events here in Summit California and Orange County and San Diego, Las Vegas for muscle contest. The number one thing that I would see was severe dehydration. And then if I would pry and ask questions, into how they got there.
I’m not gonna say all the time, but it was not infrequent for me to hear that there were some sort of prescription diuretics involved, and sometimes in very high dosages then would be indicated, for any reason. But of course you’re taking something that’s prescribed for blood pressure management or, congestive heart, Baylor management, and you’re a healthy individual and you’re taking these and you have other things going on in your system that yeah, it’s not the wisest choice.
[00:19:14] Dr Mike T Nelson: Yeah. And I’ve heard stories and rumors of people using certain drugs and forgetting that the route of administration will dramatically affect the pharmacokinetics. So if they were doing it orally versus an iv, it might be the same drug, but you’re gonna have profoundly different pharmacokinetics just by changing the route of administration
[00:19:36] Dr. Guillermo Escalante: too.
Yep. Absolutely. And then just understanding the half-life of some of these drugs, that it’s a cumulative effect. It you can’t necessarily take some of these drugs, at 6:00 AM 10:00 AM 2:00 PM 6:00 PM because hey, like that first dose is gonna be working for 12 hours, right?
. So it’s a slow continual process. And then, by the time you’ve now given two to four doses now that’s gonna be in your system for a long time. And those doses are accumulating on each other which is gonna have some potentially catastrophic
[00:20:07] Dr Mike T Nelson: effects in terms of risk management.
If someone is say, at a show and they believe someone is having any issue with diuretics. So there’s some, cuz I know you’ve worked at, several shows and seen a lot of stuff that’s happened. Is there anything in particular that someone should do because, and we’ve talked about this before, my fear is like even a lot of, e m T and very good professionals are, I don’t know if them coming upon the scene and having no idea of bodybuilding culture would think of diuretics as a potential issue just because it seems to be much more in that culture and is not something they would just run into in their normal day by day
[00:20:49] Dr. Guillermo Escalante: profession.
Yeah. I think that’s one of the biggest issues, which is why I was such an advocate of, having somebody that was in the field and even when I had this contract, I covered a majority of the events, but sometimes I would be away for vacation or I may be competing myself, and I would bring, so even though I would have another certified athletic trainer there, or even, and sometimes I would have even a another professional there.
, healthcare professional. I would actually let them know on some of the questions to ask and some of the things to look for, because you’re right, it’s not normal for a, a relatively healthy 20 some 30 year old individual to, to be taking Lasix or to be taking a, you wouldn’t even ask that question.
You wouldn’t even come to your health. Yeah. And you wouldn’t think that extreme dehydration practices are. Common unless you’re in the loop of what’s in the culture. I think of course asking the right questions is important. And asking them, for example, when was the last time you drank water?
How much water did you drink? What are you taking did you drop electrolytes or salted specifically? When, how much? When we also wanna maybe ask you might, insulin may also play a role. So maybe have you eaten carbs? Or did you take insulin? What kind of insulin, was it a slow acting, a fast acting?
What kind of insulin are you taking? So all those questions should be in there. And then you can put the pieces of the puzzle together real quick, so I know hey, okay, I haven’t had water, or I had a minimal water for the last 48. I took this diuretic and then asking what kind of diuretic they took and did they mix and match some of these?
Cuz sometimes that’s not uncommon either. They’re not just taking one, they may be combining some of these drugs root of administration is another one. And then you can put together and provide the appropriate treatment. And of course, recognizing the signs of dehydration which are a severe dehydration, which is typically, they, they’re usually not sweating much.
They have very low blood pressure. Their heartbeat is beating super fast. It’s kind of thready. They’re, they may not be with you all the time, so it’s almost like they lost consciousness, that they’re not, they may be feeling like they’re passing out, they have ringing in the ears.
So all of these things are very common. So you put all of those signs together and then you start recognizing them. And then you can intervene right away. And usually my first line of the fence is, okay well, Let’s get some fluids in you usually with some sort of electrolyte base.
So then, and then let’s get them, let’s get that in as quickly as possible. And then of course, try to get them in a comfortable position and then monitor them over time. Of course some of the athletes are very hesitant. It’s oh, I don’t wanna spill over before my show. I’m like , if you may have another show spill over, you may kill over.
So right let’s get these fluids in you right
[00:23:22] Dr Mike T Nelson: away. Yeah, no, I think that’s super useful because just in terms of, I always think of risk management, right? If more people are educated on it, hopefully there’s someone there who maybe listens to this podcast or, will know to remind, the medical professional or actually, do something there to help them.
Because correct me if I’m wrong, giving someone. Extra fluid in water isn’t gonna make anything worse, but may potentially make a huge difference in terms of risk
[00:23:51] Dr. Guillermo Escalante: to benefit ratio. Yeah, absolutely. Absolutely. Especially under those conditions. And that’s why you have to ask all those questions.
But, and if that’s gonna, you’re probably nine times outta 10 you’re gonna be right. And maybe 9.9 times outta 10, you’re gonna be right. And there’s gonna be very little detriment to providing them with any fluids at that point in time. So I think that’s important.
Absolutely.
[00:24:13] Dr Mike T Nelson: Yeah. And also I think the use of insulin is a good one too, because I did ski patrol for probably 10, 12 years. And one of the things I remember from training is if you have someone who is out skiing, snowboarding, you don’t know if they’re diabetic or not, we always used to carry like the little it’s basically like cake frosting, right?
. So it’s just a sugar you put under their tongue, depending on what if their blood glucose is too low or too high. Either way, you don’t know at that point, but if it’s too low, you could potentially save their life. If it was too high, adding that small amount of glucose is not gonna make ’em any worse.
So we just exactly did it all the time routinely, and then they would sort it out on the other end because either way you weren’t gonna make the person any worse and you potentially could. Save them in the acute
[00:24:55] Dr. Guillermo Escalante: setting. Yep, exactly right. And that’s the same thing with these fluids and regarding sugar as well.
I used to, on, in my arsenal, in my medical bag, I, I obviously had my defibrillator there. And then I also had I had some of the sugar tablets, I, Pedialyte we’re all common things that I had in there. And then I would often check, again, blood glucose levels I would check, oxygen and saturation rates, heart rate, blood pressure and then of course a asking all of the appropriate questions accordingly.
And then of course the visual inspection as I’m seeing the person and talking to
[00:25:25] Dr Mike T Nelson: them. Yeah. Cuz doing an outside medical per personnel, it almost looks like they have a hypovolemic shock. Which, yeah. Most of the time and again, this is my guess. You’re trained to think like someone, I did ski patrol.
If we see something like that and we know it’s not a glucose issue, my first thing I’m looking to see did they hit something and did they break their femur? Because if you break your femur, you could nick one of those vessels on the inside and they can just be completely bleeding out inside losing blood volume, but there’s no external bleeding or anything like that sometimes too.
So a lot of times you’re thinking like internal issue where in this scenario it could be something completely different
[00:26:05] Dr. Guillermo Escalante: too. Yep. Absolutely.
[00:26:06] Dr Mike T Nelson: Absolutely. Have you seen, again, it’s anecdotal, but in increased use of diuretics at different shows or has it plateaued or going down or what’s your, just your experience in that area?
I.
[00:26:20] Dr. Guillermo Escalante: Yeah. When I was working in the field, I would say it was fairly consistent. I would say and there were particular coaches that were known for yeah, they they’re gonna have these particular protocols and you know what those protocols are.
Those were the individuals that you had to keep an eye on. But I would say it was fairly consistent. I wouldn’t say that I saw more people using them. And sometimes some of this stuff gets recycled. You may have a year or two, or you see it less of, and then, then all of a sudden people say it’s oh you know how they used to get, shredded back in the eighties, , it was through that diuretic, and then all of a sudden you see a search.
There was actually a reason, , excuse me, posting on on Instagram where they actually posted Dorian Yates back shot, and you could see his Christmas tree in the back. And then hotty coupon’s back shot. Of course not to mention that they’re comparing different stages, different lighting, different photographers, different cameras, different angles, different positions of the pose.
Not to mention that you’re trying to compare a 2D picture to a 3D live movement, right? . So it’s not even a fair comparison of the pictures, but they were comparing the conditioning of one versus the other, and they were, the point they were trying to make as Hey, competitors in the eighties were way more shredded, way more condition, way drier than competitors of today.
So first of All those issues aside with, it’s not even a fair comparison to begin with, but all of that can add fuel to the fire because, especially if you hear the word drier, if you’re a 19 year old kid competing for your first show, I want to be dry and somebody says, Hey, let me give you some Lasix, it’s gonna really dry you out.
They’re gonna say, let’s take it, yeah. They don’t understand the repercussions of that. And then you may also have the faulty mentality of if 20 milligrams works, I wonder how much 120 milligrams works. . So then you have, a lot of issues going on with some of that.
I kind of point to say that some of these old old school types of protocols that were used, they often get recycled. And people think it’s oh, this is new. I’m like, no, it’s not new. That was done like 40 years ago. You’re just seeing it new because you haven’t been, you haven’t been alive long enough to
[00:28:28] Dr Mike T Nelson: see the cycle of it.
Yeah. Do you think some of the, I don’t know, I would say judging is quote unquote to blame because we’ve had this discussion, I’ve talked to Michelle about this too, where. I would imagine if you’re a judge, it’s easier to tell someone who’s spent, God knows how many years prepping for their show.
Maybe it’s their first show, six, eight, however many months, dieting, doing all sorts of extremely difficult things that. It’s easier to tell them you’re holding a little bit of water as opposed to you’re just not quite lean enough yet. .
[00:29:05] Dr. Guillermo Escalante: Yeah, I think that is a big problem and I think, a second line of defense into how we can make the sport safer is.
Educating judges and coaches in appropriate verbiage and terminology to use. I’ve sometimes even heard judges, some judges were probably previous competitors and some maybe may have been coaches, but not all of ’em. And sometimes you have judges who maybe don’t have a lot of background in physiology, exercise science, or even in body building, outside of being a judge giving advice on how to get the particular result.
And I think, so I think having a, providing judges a this is what your scope of practice is as a judge is basically to provide feedback and then how can we provide that feedback effectively and being careful with some of the verbiage that is used because you are right. I think sometimes judges.
To not hurt the person’s feelings, who’s been dieting for the last, four months, five months. And then you tell ’em, it’s yeah, you need to lose an extra six, eight pounds of body fat. And the person is really? Why
[00:30:04] Dr Mike T Nelson: are you crazy? What? You don’t know how much I’ve suffered.
[00:30:08] Dr. Guillermo Escalante: Yeah. And the, and that’s the reality is most people to really. Truly stage ready. At least in the in, I’m gonna talk about the men’s open division at the national level or at the professional level? Yeah, it it’s painful and it’s extreme dieting practices and it takes a long time to get there.
And when most people think when they’re ready, they probably, most of ’em could afford an extra three to six weeks of extreme practices in terms of dieting to get there, to be leaner to be competitive in the leanness component, because that’s currently what’s winning into shows is what I’m saying.
So that has a lot to do with it for sure.
[00:30:45] Dr Mike T Nelson: And how much of it related to judging too, is just the never ending push to be more extreme. Like I know they’ve, like for example, like they have a men’s classic physique now and. I don’t know if you would agree with this or not, but the first few years they had it, I’m like, oh, that almost looks slightly attainable.
Like it doesn’t look as freakish as at least the male body builders. But man, the last time I looked at the last show is I’m like, these guys look like bodybuilders 10, 12 years ago. They don’t like anything like the physique competitors or in my biased opinion of how I think it was designed to be.
It just seems like no matter what you do, everything is gonna morph towards that more extreme end of the spectrum. And I don’t know if there’s anything you can do about that other than actually changing the judging practice and not rewarding that, which is a weird double-edged sword in and of itself,
[00:31:43] Dr. Guillermo Escalante: Yeah. That, that is indeed. I think a just a a double-edged sword to say it exactly like you did because on the one end and I’m gonna, I’m gonna quote, quote Brad Schoenfeld cuz we actually talked about this when we were down in Chile. Cuz he was, Interviewed for this article in Washington News as well.
And the quote he used is, people don’t go to the zoo to see cats and dogs. People go to the zoo to see the exotic wild, the zebras and the lions and the gorillas and all of the big exotic animals, they, nobody’s interested to go see a cat and a dog at the zoo, right?
And body building is in, in the same context where people like to see the freaks in there. And that’s kinda what draws the crowd. So that being said, Because of that. It does draw the judging to be more extreme in that regard. But on the, at the same token, we also have the safety issue as to to get to this level of freakishness than more extreme practices are required.
And another analogy that I like to use is the world record in the a hundred meter dash is what, like 9.54 seconds or something like that? Yeah, that sounds about right. To see somebody run a 9.35 would be pretty awesome, but to watch somebody run a 10.05 is ah, millions of people have done that.
Yeah. So it’s the same concept where we’ve already pushed the envelope so far where, maybe changing the expectation to a more attainable state. Maybe you lose, it loses its aha moment, it loses its, it’s wow. That’s incredible.
And that’s the hard thing to balance. So it is a double-edged sword. However, I think there may be a happy medium there somewhere in between there where you don’t necessarily have to give it all up, but at the same time, you don’t have to keep pushing to those, extreme levels.
But, I just always go back cuz I was a judge for many years too. And I always think it’s but if I’m judging two competitors it’s. How are you going to judge and how do you retrain your mind to do that? Especially, so if that’s been the standard cuz we saw in women, right?
If you look at, the original Miss Olympia Rachell in the 1980s, compared to the current Miss Olympia, right? It’s a whole different look. And that evolved over time because it just, it became the norm for women to become bigger and bigger and harder and drier.
And and that kind of became the standard where, heck Rachell in the 1980s, who was Miss Olympia during her heyday, she wouldn’t even stand a chance in a figure competition, maybe not even in a bikini competition.
[00:34:05] Dr Mike T Nelson: Yeah. Yeah. And I think you even see it more profound on the women’s side, where they’ve, I think, tried to get around it by adding, more classes from body building to physique to fitness to.
Bikini. But to me as an outside observer who’s casually paying attention, it seems like the progression is still the same. If you look at the first women’s physique competitor, I don’t know when they first started that many years ago compared to now, I would be like, that looks like women’s body building 10 years ago.
It just seems like there’s this constant push towards, no matter how much they change the classes and make it, different. It seems like there’s still that drive within a, just a given period of time, because like you said, it keeps getting rewarded that you end up with something different than what I think the early intention was.
[00:34:50] Dr. Guillermo Escalante: Yeah it’s like a natural state. It’s, that’s what evolution is, right? Yeah, exactly. That , it’s like it eventually, it starts as one way and then, 10, 15 years go by or in, in evolutionary Terrance, maybe hundreds of years go by thousands of years and all of a sudden it looks completely different then.
And but that, that, that is exactly what is happening. And yeah, and I think women’s has the best analogy for that cuz even looking at bikini competitors from when they first started doing bikini to the bikini winners of today, much different figure, same thing, the figure competitors from 2000 and nine to compared to the figure competitors standing on the Olympia stage today.
Much different look.
[00:35:27] Dr Mike T Nelson: Is there anything, do you think that can be done about that? Or is that just the progression of the sport? Because like you said people wanna see freaks and all. Facets, right? I think about the, the baseball scandals with, Barry Bonds and all the stuff that happened Then, I don’t know if most fans cared because they saw more balls go over the fence.
It’s almost there’s this sort of willing part of the public to stick their head in the sand and be like, oh, I’m sure they’re all clean, but oh, they’re hitting more home runs, like drastically more. They look different, his head looks different. Oh, it can’t be anything. It’s more exciting.
We’re all good with it. But then when they find out what actually happened, everyone is paradoxically mad at the same time. .
[00:36:11] Dr. Guillermo Escalante: Yeah. And to me that’s the disturbing part is, people often wanna see the extremes of things, but they don’t necessarily wanna. What is required to get to those extremes?
They just want to see the end result. They don’t want to see the steps necessary to get there. And that requires, people call bodybuilders or even, any, anybody who’s the best at anything, they call ’em, they, if most people would call ’em, they’re obsessed with something because you are.
There is no. In being a world champion? No it’s it’s a job 24 7. And if read anybody’s story that’s ever achieved, top level of success in whatever it is, even if it, a multi-billionaire, probably unless they won, the lottery several times, chances are they’re a workaholic and they’re, that has been their life passion.
And same thing for an athlete and for a bodybuilder to, to reach the Olympia stage, that is their life. There, there is no necessarily an off button to be able to do that. And a lot of things that go behind the scenes
to
[00:37:07] Dr Mike T Nelson: get there, it seems to me like, talked about Dorian. I remember the first time, I think I saw a video of him.
Was it the Grand Prix? I can’t remember. Where, to me watching him was like, holy shit, this is like a whole. Another era. And I think part of that was the way he trained. No one saw pictures of him. There wasn’t the internet back then, like there is now. Like I think he had the ability and obviously had an incredibly freaky physique, very dry, conditioned, all that kind of stuff.
But I think the fact that he showed of showed up out of nowhere that to me it just seemed like at that point everything got much more extreme than what it was before, and it was already very extreme. I don’t know what your thoughts are on
[00:37:55] Dr. Guillermo Escalante: that. Oh no he’s definite, Lee Haney was an amazing champion.
Uh, Oh yeah. And he, and obviously he’s the whole title for most Olympics in a row. But after the Lee Hena era came, the Dorian Yates era and that’s when you see, a sharp change in in the evolution. Of body building. And then of course, after him, then came Ronnie Coleman, and then Ronnie Coleman took it to a whole new level.
Even Ronnie Coleman, when he won his first Olympia to Ronnie Coleman, when he won his last Olympia in terms of his muscularity and everything, even though, personally, my favorite Ronnie, was in that probably 99 2000 area, . But he continually got bigger and bigger and still came in, in, in condition, in good condition.
And that’s just everything was just, everybody was just chasing that, right? And I, and I love some of those physiques of the 1990s and early two thousands with, Kevin Labron and Sean Ray and gosh, just Flex Wheeler, watching some of those guys over the years was amazing to see them.
But but yeah, just looking at those people that I just mentioned, for example, lot of ’em were just so in, in such incredible shape and condition and by today’s standards, they’re actually be, they’re rather small compared to what some of the competitors are up there today.
[00:39:02] Dr Mike T Nelson: Yeah. It seems to me like there isn’t much difference from some of, at least on the male side, from some of the top physiques now. And again, I don’t follow it as much as I used to, but it seems like that just has disappeared. Like even to go back to the time of, Arnold, where you had Arnold, you had Franco, you had Zane, you had people who had very different looking physiques that all, placed well.
And then even back, like when you were talking about with everything from Frex wheeler to Ronnie, to even Jay Cutler to it, did it seem like over time they all started morphing and looking very similar? We’re now. I don’t know. They all just, maybe I’m too much of an outsider, but they all look very similar now compared to what they used to.
Maybe I’m just one of those two old school people that’s back in my day when I was watching it, type thing. .
[00:39:51] Dr. Guillermo Escalante: Yeah there’s definitely been a lot of again, like an evolution in the sport and in what we see up there and really what qualifies And then obviously what wins?
I will say this year big Romi took fifth place and he’s by far the biggest competitor there. And I think top two were Derek Lansford and and Hotty. And realistically, I think if I had to put money on it, I think they were probably on the lighter side of the competitors.
But they’re also relatively shorter, , to compare to some of those guys. They. So in terms of muscularity, they were still big, of course, but compared to Rami, he had more beef on them compared to Brandon Curry. He had more beef on them too. They just were a little bit more symmetrical, flowed a little bit less, less gaps in their physique.
And then of course they came in better condition which is, I was glad to see them win. And I thought they showed up very well in, in presenting a good package. But so yeah, so in that regard, it was a little bit different because it, it was a war rewarding big Romy and I am one of his fans.
I like him as well but his physique is very different. It’s more on the mass heavy side than it is on the other components of
[00:40:56] Dr Mike T Nelson: the judging. Yeah. And then it seems like there’s a common belief, maybe it’s not common, but that. If I took the same drugs as what these top competitors are doing, that the drugs just do all of the work for you.
And I think of the Louis Simmons quote who granted it’s power lifting, but he was from me as an outsider looking, probably one of the first guys I ever saw that was like, yeah, we use drugs. And he was very open about it. And I was like, whoa. Oh my gosh, how is that possible? And I remember someone asking him in an interview and he’s yeah, I got a gram of testosterone in the back and a denim shirt.
I haven’t seen it lift shit so far. , and his whole thing was that yes, we are using a lot of drugs, but it, the drugs aren’t doing all the work where it seems like an outside perspective would be if I was using the same magical whatever cocktails these professionals are using, then I would look the same as them.
But you go back and you look at pictures of. Ronnie Coleman, for example, his first show where he was, natural, he was crazy looking like Lee Priest when he is 18, 21 years old. You’re like, what the hell is that? Like these people were, Kai Green competed for years as a natural body, but they’re in tested divisions.
I think people don’t understand that these guys were freaks before they, did anything in terms of enhanced competi.
[00:42:19] Dr. Guillermo Escalante: Yeah, I think that’s a really good point to highlight, especially for the listeners that are on the younger side, maybe are aspiring bodybuilders because the drugs aren’t every, I’m not gonna say that the drugs are more than sprinkled on the cake, but they’re not the whole cake.
The foundation of the cake still starts, number one is who are your parents? They’re genetics. Yeah,
[00:42:36] Dr Mike T Nelson: genetics, genetics are gonna play the largest role.
[00:42:39] Dr. Guillermo Escalante: Huge. Of course you can maximize, whatever genetics you have through then proper kind of the second layer foundation, which is, appropriate eating and fueling your body appropriately.
And using appropriate training programs and methodologies to, to maximize your gains in that regard. Of course, then implementing getting in enough sleep and getting that life pattern component. All of those are so important that I think are often minimized. think.
If you’re up partying and drinking, if you’re not sleeping, if you’re inconsistently hitting the gym, if you’re not necessarily getting enough enough nutrients into your diet, micronutrients and macronutrients cuz that’s another thing. People focus so much on the macros, they forget the micros.
And it’s Hey, those are important too, guys. They play critical roles in in your body actually functioning appropriately and getting maximum results. So putting all those things together, getting enough nutrients in you, all of those are gonna be very important. So I don’t care how many drugs you take, if you’re not doing that foundation, it’s not gonna work for you.
So it really takes everything together to be able to do that. And you’re right, some of these individuals they’re already gonna be the biggest, strongest people naturally. And if we go back to the home run era it’s the same thing. Barry Bonds and Mark McGuire, all of these guys, They were amazing athletes and baseball players before they even decided to jump on the juice.
Yes. The juice basically added a little extra spice to their ability to do that, but it didn’t make them a pro baseball player. Yeah. They were of that caliber well before they got there. And that being said, sometimes individuals, we’re so different that some of these people that are so gifted already, It doesn’t take a whole lot for them to Yeah.
Get to these extra benefits. Whereas some people, it might require a whole lot and some people may have a lot of side effects, taking a little bit of stuff, and other people may be able to take a lot of stuff without a lot of side effects. So there’s a lot of inter-individual vari variability there.
And yeah, just because you take the exact same stuff that some of these pros take is not gonna g. That you’re gonna look like that. And in fact, there’s a lot of people that try and they fail very miserably because just not the equation that they’re gonna get there. Even training practices, when you see some of the training practices, some of these top bodybuilders, sometimes some of ’em don’t even train very efficiently in my No.
Or smartly, but it doesn’t matter because they’re the type of people that walk into the weight room and all of a sudden they’re swollen. They don’t even need to lift the weight. They just kinda walk in. Of course I’m being facetious there, but they could do anything and, and they would grow.
Whereas a lot of people, it takes more methodical programming to be able to do that. And we see that even in our studies, right? We see hyper responds and we see non-responders using the exact same training program or the exact same supplement that you’re providing them. And you’re gonna see people that respond very well and some that maybe even.
Respond poorly, where they actually decreased their performance doing the exact same protocol so the same’s gonna hold true with these anabolic substances.
[00:45:41] Dr Mike T Nelson: Yeah. The first time I saw that was got a C S M in 2005, 2006. Stu Phillips was there presenting on, one of the studies looking at a hypertrophy study.
And I’ve talked about this in the podcast before, but he puts up a nice scatter plot of all the data that people, I think it was like a 12 or 16 week study, I, maybe it was a little longer. Most of the people are in the middle, right? They gained a few pounds, did pretty good. There was two people who were like two standard deviations, like almost off the top of the chart.
And then there was one poor bastard who got worse . And it was super funny cause they asked what’s with these two people way at the top? And that’s what kind of responded, why they did some studies looking at acute testosterone release and growth hormone and a bunch of other stuff. But to me it was just fascinating how.
They did the same program. Granted nutrition wasn’t extremely controlled. They were told to eat the same thing, but they weren’t, living in a lab or anything like that of how you can see such dramatic, results. And a buddy of mine who worked for one of the muscle megs for years and trained with some of the top pros, and he said in his experience that, he said one of the guys was Paul DeLeT would come in and train at his gym.
And he’s I don’t think I ever saw that guy do more than 60 pounds of tricep press stones ever. And his arms were just massive , right? It just seemed like he said some of the top pers that train there. And again, this isn’t all of ’em by any means, that if they just put any tension on the muscle at all, they got a response where some other people have to do something completely different.
Maybe it’s a higher intensity, a lower volume, higher volume, whatever. I think. There’s so much variability in something like hypertrophy and then you add, like you said, drugs on top of it. There’s people who are probably hyper responds to small amount of drugs. There’s probably people who can take a shitload of stuff.
And I’ve seen some blood work on people who told me what they were taking and I’m like going, oh my God, this is, they’re gonna have an H HDL of freaking four. And it was fine. I was like, you there, you what? There’s no way. And someone else doing an H R T dose, they’re, their HDL was 11.
He was like, what the heck? , just, again, very limited case studies, but just massive amounts
[00:47:45] Dr. Guillermo Escalante: of variability. Yeah. And there’s a ton of that and I think a lot of people don’t understand that component. And not only that, but. . It’s again these these performance enhancement drugs give the person the ability to actually push harder, train harder.
Yeah. Recover faster. So it’s actually not to do less. It’s actually to be able to do more and recover faster. And and that, that’s basically what helps in the process. So if you add all of those things together, and now you have somebody that’s genetically gifted, who is doing the foundation of the diet and the training and the sleeping and the consistency and taking their time, and then you add the dietary supplements and then you add the peds on top of that, then all of a sudden you get Mr.
Olympia. That’s what you get.
[00:48:32] Dr Mike T Nelson: Yeah. And last point on this, and we’ll talk a little bit more about some of the risks is taking. Advice from genetic freaks who are maybe using and making choices you’re not making for someone who’s starting out is probably not the best direction. But that’s like the history of most especially old school muscle magazines.
I remember Lee Priest complaining that he is oh my God, like all these muscle magazines, they just want me to do another arm article. He’s I don’t really train hardly any different from my arms over the last 15 years. And you look at him and you’re like, how is that even possible to have arms like that?
Yeah. But he was a genetic freak. Obviously. He trained hard, but he didn’t use a lot of ride. He didn’t do a lot of crazy shit. But you see a picture of his arms and, to 18 year old me, I’m like, how’d he do that? ? Yeah.
[00:49:16] Dr. Guillermo Escalante: What’s your secret? what he would tell you is probably extremely disappointing.
a young kid, you’re like, you mean you just do bicep curls with the dumbbells and Yeah. Bryce cable press downs with the tri, with the tr for
[00:49:28] Dr Mike T Nelson: triceps. And you and your right is doing that twice a week. Week, yeah.
Yeah. I remember the other part too, was that a video, Jay Cutler was talking, he is yeah, straight bar bench press isn’t the best for your peck growth. And then later in the video they’re asking and what did you do? What was your history? So the interview asked a very good question, what did you do when you first started?
He’s I found dumbbells are more effective. But he is in the hike high school I was benching like 4 0 5 for reps. I’m like, what the hell, ? I’m like, yeah, that might be more effective if you’re a freak benching 4 0 5 for reps in high school already. Like a straight barbell may not be the best choice for you.
But for someone who’s listening, who, like me in high school, got squished by an empty bar, yeah. Barbell bench press would probably be pretty helpful for me. . Exactly. So you published an article looking at some of the autopsies of some bodybuilders, and it just seems in the media, maybe it’s because of the internet, maybe we have more exposure to people.
Maybe we know more about these things than we did before, but at least to me, it seems like in the last five years or so, the amount of deaths in body building in general seems to be more of a escalating, and especially people at a much. Younger age. I know Bill Pearl unfortunately just passed away recently, but it seems like the people who did it many years ago have, been able to live relatively long life where we have a lot of people who are much younger, sooner younger, appear to be passing away much sooner than in the.
[00:51:04] Dr. Guillermo Escalante: Yeah, that, that’s definitely what we noticed as well. And really what kind of caught my attention was right around 2020 2021. Dallas MCC Carver caught my attention. Yeah. Daniel Alexander caught my attention. He, he was 30 I remember he competed as a middleweight when he won the U s A championships, and I followed his career and, he died at age 30.
[00:51:24] Dr Mike T Nelson: He used was Dallas even 30. How old was he?
[00:51:26] Dr. Guillermo Escalante: He was very young. Yeah. Dallas was only 26 when he passed away. Yeah. Yeah. And then John Meadows, is 49 man and the list goes on. And of course, and there were some that died relatively young that, we actually made our cutoff at 50.
Okay. So what we specifically did is we basically just did a very generic Google search to see what, where do we, where can we find individuals who have reportedly died? Of some of any condition, first of all. And then we eventually narrowed the search down to people, body billers who had died, body billers, who had died, who were under the age of 50, between the years 2010 to 2022.
We did the search in February of 2022. And then we started narrowing and filtering down. Ultimately we, we really wanted to find the autopsy reports of these individuals. Cause we wanted to see, okay, are the re are the reported cause causes of death? Because they weren’t in medical journals necessarily.
So are these reported causes of deaths actually, The actual reported causes deaths that the coroners reported. And we started narrowing the list. Of course we had to narrow it down. We had people from all over the world, from Italy, from from great Britain who had passed away. Of course we can’t get autopsy reports for those individuals.
At least not easily. So we were able to narrow it down to people in the United States who had that. And then we actually finally started calling coroner offices. So we had a large number of individuals who had actually passed away over 40 worldwide. And then by the time we got down to the U S A, it was that were under 50 that were related to either some court, some sort of cardiac condition or an unknown condition cuz we wanted to investigate that further.
We included that in our search. And then we had about 14 that we narrowed down to for that point in time. Then we called the coroner’s office where we were able to try to get the coroner reports we’re actually able to get seven coroner reports from those individuals. So that’s basically what our analysis is based on.
Unfortunately, one of those individuals did not die of a heart related issue. It was actually a suicide. So we disregarded that. Cause our focus was on cardiovascular related events. However, it’s should be noted that there is some research to suggest that brain health and depression are an issue.
So it shouldn’t be ignored completely because that is another study in its own really is looking at the potential. Mental side effects that it may have over time, particularly when they’re coming off cycle. There is, again, very preliminary evidence to suggest that there may be some sort of link there.
Hard to identify a true cause and effect, but there is something that, that I think should be investigated further. But we focus on the cardiovascular related events. And you know what we found was there were some common threads that were in a lot of these reports. Before I go further, I wanna say there were definitely some limitations in the way the coroner reports were written.
We actually discussed that in our discussion because a lot of the coroners maybe didn’t necessarily identify these individuals as potentially using performance enhancement. So the coroner reports weren’t necessarily extremely thorough. So not all of ’em had toxicology reports. Not all of ’em did a lot of extra testing that maybe would’ve given us more information.
Couple of them were quite thorough but the majority of them were not. But we did see some common threads in what the what the report showed. We actually did an average of the hearts. All of ’em had an enlarged heart. And actually the enlarged heart was about 74% larger than the reference man.
But that’s substantial with a grain of salt because I do like to say they’re bigger. Yeah, we did re use the reference man, because that’s what’s more readily available. Ideally it would be good to compare it to other non-drug using bodybuilder. But obviously you’re not gonna be able to weigh the heart of , right?
Of living non-drug using bodybuilders. So it was an impossible ask. So as a result of that, we use the reference app because there is cardiac hypertrophy reported even with healthy non-drug using weightlifters. But nonetheless, we don’t see those guys dying necessarily. So we, that’s where we always have to of look a little further.
We also saw that the left ventricle was actually significantly larger as well as compared to, to reference men of their age. So a lot of interesting facts. And then obviously we see a lot of these common things. We see basically atherosclerosis at very common thread among all of them.
We see cardiac hypertrophy, cardiomyopathy, we see lept ventricular hypertrophy. So we see a lot of these different red flags that kind of keep appearing. Some actually had some history of where you actually see, yeah, th this person had basically low h d l high l d l. So you have this lipidemia going on in
[00:56:07] Dr Mike T Nelson: some of their So low hdl high L D L you mean?
[00:56:10] Dr. Guillermo Escalante: Yes, exactly. Yeah. So we have, so we have a bad ratio of the H D L and the L D L ratio. And we see just some common threads all the way across. So it was very interesting to actually see and at the end of the day, we basically said we can’t put a cause and effect on all of this stuff, of course, but we also can’t ignore the smoking gun and we need to investigate further into what is going on.
We actually did reference several articles in the discussions that have actually. At practices of some of these bodybuilders that are natural compared to non that have actually been using. And they’ve actually measured, of course, they’re not prescribed this stuff. They’re actually, they’re self-medicating themselves.
And then they choose to be in a study and they’re looking at, for example, what happens to to their heart, to their ventricles, et cetera which happens to the, to their blood lipids over time. And typically what you do see is again the L D L level does typically go up. H d L level does go down over time.
And then we do see again that cardiomyopathy seems to appear quite a bit with some of these individuals.
[00:57:11] Dr Mike T Nelson: And part of that related to cardiac issues, do you think that’s made worse by potential? Diuretic use. So I think of, so testosterone for example is well known to increase blood, red blood cell mass, right?
So you’ve got basically more red blood cells going around and then now you’re trying to do dehydration practice on top of it. I think of some of the cyclists from the tour of France who’ve had hematic grids that are just absolutely scary. For other reasons, they’re probably primarily using E P O and other things to drive up red blood cell mass.
So they have better endurance performance. But there’s been case studies in there and reports of, cyclists getting up at three in the morning to go exercise just because they felt like their blood was getting a little bit too thick. I know that would be something that would be harder to see on an autopsy though.
Correct. In terms of multifactorial reasons related to cardiac.
[00:58:09] Dr. Guillermo Escalante: Yeah I don’t think you wouldn’t necessarily see it but there’s definitely a lot of truth with that. And this is why one of the things we were talking about earlier was you’re absolutely right. Erythrocytosis is very common with these individuals.
And that’s because you’re gonna get, increased red blood cell production from the, a lot of these performance enhancement drugs. So now you already have, more more absolute red blood cells in there making your blood essentially a little bit thicker. And then now you dehydrate the blood plasma, which is, 70 plus percent water.
But now you deplete that, but you still have this, these thick red blood cells in there which is gonna potentially create larger problems. And this is where I see the complications, where I think people don’t put all of those things together. It’s Hey, like I’ve been, I’ve been taking these performance enhancement drugs, for the last.
Six months or six years, whatever the case may be. And then, I have a, a larger red blood cell count. Now I’m gonna basically dehydrate my body, which also includes my blood plasma, making my blood thicker. So now you actually have absolute erythrocytosis at that point in time or I’m sure relative erythrocytosis at that point in time.
So you have a lot of issues going on at that, at in there that are combined with all of those. And then you may be taking the albuterol, you may be taking the ephedra, you may be taking the caffeine and you may be depleting your electrolytes. So all of a sudden you have way many more factors that are contributing to the danger of of exposing the individual to dangerous practices.
[00:59:38] Dr Mike T Nelson: And I would, we don’t really know anything about blood pressure or history or anything on these individuals, do we? Cuz I would. Imagine if you’ve got left ventricular masses increasing. Do you think some of that is from potentially the drugs? Do you think some of it is a side effect of having high blood pressure on top of it, on top of having a higher red blood cell mass?
So just the amount of physical work the heart is doing is more than what would normally be required of it on top. Potential effects from the pharmaceuticals?
[01:00:13] Dr. Guillermo Escalante: Yeah, I think there’s, we do see a lot of hypertension in these individuals and it’s not uncommon. In fact, when we did some testing.
I have an article coming out in journalist Strength and Conditioning research, but we actually see some individuals with relatively high blood pressures at some point in time, and some of ’em are dehydrated. So that’s their blood pressure being low, which if they were not dehydrated, it would actually be higher.
And in my lab we actually, I haven’t published this paper yet, but I have data of individuals that came in at different points in their contest prep. And then we would actually measure the blood pressure and they actually answered a survey and we actually looked that out. What kind of drugs they were using.
What kind of dietary practices? Training for everything. You actually see some individuals where I would actually be testing their blood pressure and I, I would see it as elevated. So I would of course let them just rest and relax for a little bit and retest it. And retest it again. And, I would see 20 some year old guys, 30 some year old guys with hypertension.
And I’m not talking like just a little bit elevated, I’m talking. 180 or 200 over one 40, so
[01:01:19] Dr Mike T Nelson: that’s significant.
[01:01:20] Dr. Guillermo Escalante: It’s high, right? Yeah. So my next step is hey, you should go to the doctor, get this checked out because this is really high. I’ve checked it, and maybe you’re just nervous, but sure we should get this checked out.
But of course I would pry and ask them with regards to what kind of performance asthma drugs are you taking? And then you see the picture kind of forming and and yeah. And unfortunately, what I like to say I was saying this again to Eric Helms just the other day is I use the terminology look under the hood, and looking under the hood means getting regular blood work.
Not only when you’re off cycle, but also when you’re on cycle. And so if you’re getting it only once or twice a year is probably not enough. I recommend three to four times a year work with a medical professional to help you interpret that blood work and have a history of that blood work with you so you can track things over time.
Check your blood pressure regularly and regularly, even on your own, you should probably check it, at least. Couple times a month, maybe even weekly to keep a marker on what’s going on with that. And if it starts to trend upward, go see your doctor and see what’s going on with that.
Checking your blood glucose levels and making sure that those, because sometimes people are taking human growth hormone for example, and that may actually make you have hyperglycemia at that point in time. We wanna make sure that we’re monitoring your blood glucose levels that regularly.
So all those things, those are very easy preventative measures that can be done by the individual. So checking under the hood on a regular basis is something that’s not done. And if they do check under the hood, unfortunately they only check under the hood when they are off cycle, which you’re missing the whole picture because.
Things should be back to normal. At least you hope when you’re not on stuff. But if you’re on stuff nine months out of the year and you’re off stuff three months out of the year and you’re only checking it, at that six weeks after you’ve been off pings when things are back to normal or at the tail end of that three months when you, now you’re giving your body three months to come off of all the other.
But you’re on the stuff nine months out of the year. You need to look into the hood when you’re actually on everything to see how your body is responding, managing, because that’s really what your insights are starting to look like over time. And again, the issues with these drugs is it’s a dose response relationship, which is related to quantity.
Of course quality, cuz there are a lot of ’em are getting underground stuff that’s not necessarily good. And then of course, length of time o of exposure that they’re doing it. So if you’re doing super high dosages with low quality stuff for long periods of time you’re gonna, you’re gonna be in for some trouble very soon.
[01:03:48] Dr Mike T Nelson: Do you think part of it could be further impacted if you were not doing a lot of, cardiovascular training? Because in essence you’re rewarded for training for hypertrophy. Now I know obviously body billers use cardiovascular training as a way to, lose fat and burn calories, but. It again, maybe I’m skewed from looking at muscle magazines, but you don’t ever really see, top X competitor, oh look, here’s this cardiovascular routine.
If you do, it’s here’s what I do to burn fat. That it seems like cardiovascular health is not top of mind awareness, and maybe that’s because they’re not necessarily being rewarded for it. So you’re doing we know at least acutely from some studies on, weightlifting, that blood pressure can spike up pretty high during weight training, which again, doesn’t mean weight training itself is bad.
But I just think about the constant force, the left ventricle would have to create against a high pressure when you’ve got, under tension and that being compounded potentially by different pharmaceutical practice, maybe in lieu of only doing cardio before a show. I don’t know if you have any thoughts on that as.
Potential risk factor on top of
everything
[01:04:58] Dr. Guillermo Escalante: else. Yeah, no, I think there’s a lot to be said to that. I think I’m gonna, I’m gonna even go one, one slight step further and looking at these old practices of bulking to extreme levels, and then, yeah. And then cutting to extreme levels so that you have this huge shift, if you’re staying within 15 ish pounds, 20 ish pounds of your competition, body weight that’s probably about the maximum that you really need, to, to really to really succeed.
If you’re putting on and what I’m saying is if of excessive body fat, right? If you’re putting on quality muscle mass, but you’re not gonna put on 30 pounds of muscle in a year. I don’t care what you’re doing, right? No. If you’re adding, if you’re a, if you’re having a lot of a, adding a lot of body fat in that point in time, and obviously if you’re doing that, they’re typically less active.
They’re still gonna be weight training, of course, but they’re typically not gonna be doing the aerobic training. So you have this. Two things working against you and I think keeping that into per in perspective is really important in terms of keeping your body fat in check and how can I keep my body fat in check and my heart healthy?
I can actually implement some sort of aerobic training into my regular training routine, even if it’s three or four days a week at a moderate to low intensity. Just to help manage both of those things. Cardiovascular health as well as the body fat management. And of course, you don’t necessarily wanna overdo it either because then you know if you’re doing an hour of cardio, Six days a week in your off season, then where can you go when you begin your cutting, right?
Yeah. You’re gonna, you’re, if you’re gonna implement more cardio, you’re gonna be doing hours of cardio. Finding that sweet balance is really good. And to me, just a minimum dose of, maybe about hundred to 150 minutes a week of a, of aerobic exercise doesn’t have to be even high intensity, but at least getting out, doing some walking doing some lights, stair climbing bicycle riding can go a long way.
[01:06:49] Dr Mike T Nelson: Yeah. I seen in my power lifting friends who go up a couple of weight classes, as they get to the end, they’re like, yeah, the only thing that’s good is lifting weights. Everything else just sucks. And the, the handful of ones who I think have done it a more intelligent manner are watching their, their blood pressure, their blood glucose.
You, you tend to see this exponential thing where they’re good, and then. All of a sudden towards the end, everything is just going haywire. Yeah. And I’ve even seen that in friends of mine who are natural competitors for body building. Like they’re doing good, everything is good.
They’re, six weeks out from a show and like their blood chemistry is just fucked, for lack of a better word, . And they’re not even using any external compounds. It’s just the stress of trying to put your body into a state that it just doesn’t want to be in period, I think is something that people.
Forget about that is just doing it and of itself is a massive stressor on top of everything
[01:07:44] Dr. Guillermo Escalante: else. Yeah, absolutely. And that’s very common. Like you said, it’s just whether you’re a natural or not, but even things like your sleeping patterns, and everything else. They’re extremely disrupted where, it’s like two hours of sleep is like a success sometimes in when you’re, three weeks out from a show.
And it’s not because you’re not trying to sleep, it’s just because you literally can’t sleep. You’re hungry, you’re uncomfortable, you’re your body is going and maybe you’re taking other stimulants, like even natural stimulants, right? Or a legal stimulants like a caffeine, right?
You’re just constantly going. So yeah, it makes it very
[01:08:15] Dr Mike T Nelson: difficult. Yeah. Our friend Eric Helms, like the best phrase I got from him, he is, Oh, you mean body building? He’s you mean competitive starvation, ? Yeah. Yeah, absolutely. I was like, oh yeah, that’s a good one. .
[01:08:28] Dr. Guillermo Escalante: No, it is. And to get to those levels of winning physiques, it, it’s it takes a lot and you have to there’s a lot of suffering involved, that’s for sure.
And a
[01:08:36] Dr Mike T Nelson: lot of sacrifice. How much do you think just the combination of, I think of GH insulin and, anabolics to me that, and again, if you look at some of the physiques they look at in terms of, intestinal growth and, guys can’t do vacuum poses like they used to. And it just seems to me that would be a, an exponential risk because there’s no real point in physiology where all three of those are all elevated at the same time.
So now you’re just of promoting. Not even muscle growth, but just growth of all tissues almost at all costs. And like you mentioned, the cardiac system. Cause it’s enclosed in basically a small bag doesn’t have anywhere to go, so it’s gonna go inward and your thickening of the chambers are gonna get bigger and that’s gonna obviously reduce the amount of, blood flow and add more cardiac stress on
[01:09:29] Dr. Guillermo Escalante: top.
Yeah, no, absolutely. And they do all play a role in, in that. And in fact, that’s one of the goals of, of competitive body builders is hey, like what’s your IGF level? Yeah. And the higher, the better in, in terms of muscle hypertrophy or actually just hypertrophy in general, but there is, again, you walk that fine line where too high can lead to other deleterious side effects that you really don’t want.
Yeah. You may wanna run it high, but not so high where you’re having all of these other potential side effects. But how do you achieve that Is basically by exactly what you said. You put all of those variables together and then you’re able to increase that IGF one.
[01:10:08] Dr Mike T Nelson: Yeah. Last two questions as we wrap up.
In terms of, words of advice of people who are. Considering, say, enhanced body building. My, my 2 cents is the good and the bad is that it’s becoming, I think, use of drugs is to become more accepted. We can argue if that’s good or bad. I do think it is easier than ever to try to get higher quality information.
I don’t know what your thoughts are on that. My bias is everyone should be free to do what they want. And again, your, if B for example, doesn’t test for steroids, so you’re not breaking any rules in terms of the competition. Other competitions are obviously tested competitions. But my goal is that hopefully people would be more educated.
They would seek people out like yourself, read the literature and try to determine themselves, okay, here is my risk analysis ratio. And after putting thought into it, Hopefully we’ll make a more educated decision. But it also seems like there’s a never ending push for, like we said, just to see, freaks at all costs.
And I’m sure there’s people who unfortunately still go into it, rather uneducated about here’s the pros and here is the
[01:11:23] Dr. Guillermo Escalante: cons also. Yeah, I think for me, the number one thing is educate yourself appropriately do understand that there are risks associated with this. So make sure you understand fully what those are.
Read the medical literature and heck, everybody’s got access to pub nowadays, or at least Google Scholar. And maybe not all articles are accessible. There’s a lot that are free access. And you can definitely read a lot of information. And I’m talking firsthand information.
It’s not necessarily opinions of professionals in the medical field, but it’s actually people that have looked at investigations and, done studies and they’re. Just reporting the data. There’s, they’re not trying to sell a story. They’re just basically reporting data on this information.
So you can actually see, all of the potential side effects that may come, on the cardiovascular system on the liver, on the kidney, on the brain. And then of course, maybe even aesthetically, I’m thinking for women, things like, your voice deepening clitorial enlargement for men, maybe acne all of those things are gonna be things that you probably wanna consider.
Understand, which ones are gonna be reversible and which ones are not. And there are certain side effects. You reach a point of no return. And like for women specifically, once your starts, starts to deepen, that’s your new voice now, right? Those are the things that you wanna consider.
There are a lot of things like obviously for the liver, for example. Obviously if you’re taking a lot of oral compounds your liver’s gonna be more taxed than if you’re doing injectable compounds. Those are some ways in which you can do that. And obviously once you stop doing the compounds and that’s gonna decrease, you’re dyslipidemia for example, that’s something that does reverse once you come off some of those things.
But it’s one of those things where if you’re. If you’re constantly on, and that dyslipidemia stays for years and years on end, then that could potentially lead to the atherosclerosis, down the line later. So I think you should definitely be educate yourself into the true risk and the and and of course there, there are aesthetics positive effects and performance benefits.
Of course, there are benefits. That’s why people are doing them. So you need to make sure that you’re weighing that you wanna weigh in on the legal aspects, right? Because there are legal repercussions for some of this. These are illegal substances, if you’re, buying them, from underground market or whatever your source is, there may be some potential legal repercussions for that.
Work with a professional a licensed healthcare professional, work with a p. Be sincere with them and find. And if you can’t have a conversation with them openly, then find one that you can have a conversation openly with. They can probably help educate you in some of the risks associated with it if they’re in the in the know of of the industry a little bit.
And they can probably help guide you, not necessarily what to take, but maybe in how to mitigate some of those risks and how to manage your risk and how to look under the hood and follow your history on a regular basis so they can actually, guide you into, Hey, look, this is what’s, this is what this, you started this and this is the result of that.
This is what’s happening internally. So you cannot help understand that don’t try to interpret that yourself. You’re not a physician, right? That’s what doctors are for. So I think there’s a lot of those things that you can definitely do and understand and obviously don’t be a SLS bag and compete in a untested, better in a tested federation and say that you’re drug free when you’re doping up, if you’re gonna, if you’re gonna decide to cross the line and compete as an enhanced competitor, then compete in like what you said, Mike the divisions that don’t test, right?
Yeah. So that way the ethical part is not really there because. You’re an even playing ground. Everybody is basically choosing to either use or not use. So let the natural competitors be natural and compete. If you wanna compete naturally, then compete in the natural federations. If you wanna utilize, compete in the untested federations and that’s your choice.
And to me, that, that’s one thing that drives me nuts is when people claim to be drug free and they’re not. And they compete in the tested federations and try to cheat the system because at that point in time, really what’s the point? So if you wanna compete and compete with the people that are using, they compete with the people that are using the performance enhancement
[01:15:25] Dr Mike T Nelson: drugs.
Yeah. Yeah. I’ve never understood that. So you’re gonna use drugs to win in the natural competition, but you just violated the whole rules of why there’s a natural competition to begin with. It’s like I. I, I’m sure people will try to do it just to say they won whatever, but yeah, I don’t, that boggles my mind, .
[01:15:46] Dr. Guillermo Escalante: Yeah, absolutely.
[01:15:47] Dr Mike T Nelson: Absolutely. Yeah. And that’s a good part about as of right now in the US of this recording, like most of these drugs are illegal and they’re not like, I think they’re still schedule one, I think, aren’t they for the most. Schedule three.
Schedule three. Okay. Schedule three.
[01:16:02] Dr. Guillermo Escalante: Yeah. But yeah, so you, even and even if your doctor is, because they’re highly regulated if you get, if you’re, if you have a physician that’s prescribing you, testosterone for example, you have to show your identifi identification and everything.
It’s very tightly controlled with all of that. And that’s the other thing, with the t r t a lot of people confuse this thing. It’s oh, I’m just on t r t. And it’s t r t is like for a clinical diagnosis of a medical condition. If you’re loose using low dosages of testosterone to enhance your perform, You are using performance enhancement drugs.
You’re not on T R T. Somebody who’s on T R T is just basically taking enough testosterone under physician or medical supervision to get their levels to a normal healthy range, not to super physiological levels. If you’re a 25 year old kid or individual taking 200 milligrams of testosterone and you’re not on T R T, you’re a performance enhancement drugs because you’re gonna be at super physiological levels
[01:17:00] Dr Mike T Nelson: at that point in time.
Yeah. It seems like some people saying they’re on T R T is just an excuse for them to be using super physiologic levels, which I think even unfortunately makes the education and everything worse, right? Yes. Because there’s a huge difference between taking a replacement dose to be back into a normal range versus, if you’ve seen blood work on people who are taking very large doses, you are.
Not just a little bit outside the range, A lot of times you’re in a different ballpark somewhere else. in terms of that
[01:17:32] Dr. Guillermo Escalante: range. Two to three standard deviations above that range.
[01:17:36] Dr Mike T Nelson: Yeah. . Yeah, . And it’s a good part too about the legality of it and then, because a lot of ’em, if you’re obtaining it through illegal means, not only do you have the law issues, potentially ethical issues, you’ve got purity issues.
A lot of these are injectable compounds, who knows, like where you bought it from. A lot of those people, there’s not a huge incentive for them to be doing the world’s best pharmaceutical grade practice in terms of sterility, making sure what’s on the label is in there, all that kind of stuff.
Like you’re in the wild west with, whatever. Dude recommended on top of
[01:18:10] Dr. Guillermo Escalante: it. Yeah, absolutely. And also, unfortunately another thing that’s become apparent is that some of the coaches are also the drug dealers in terms of some of these things.
And there, there’s an inherent conflict of interest, right? Because if you’re making more of your money on the sale of these compounds, then you want the individual from a business perspective. I’m not saying this is the right thing to do from a purely business pers perspective, you want people to buy more, not less, right?
You’re not necessarily gonna try to give the minimal effective dose. It’s no, get as much as you can because if you’re trying to make the money, that’s what you’re trying to do. And, and there, there are those ethical boundaries there that you have to be be careful with. Yeah, it’s important.
And you, like you said you hit it on the nose, the sterility issues the purity, these compounds, they can be very compromised. And just because, The label looks nice and the it’s, it says it’s got X amount of whatever. Doesn’t mean it says, it’s pretty cheap to create an nice looking label and an nice looking vial.
It’s, it takes a little bit more knowledge to actually manufacture that in under, pharmaceutical grade compounds that are not gonna
[01:19:16] Dr Mike T Nelson: harm. Yeah. And some drugs like clenbuterol, you’re talking micrograms, not milligrams, micrograms of a drug. The last I knew of was never approved in the US
[01:19:27] Dr. Guillermo Escalante: So yeah. It was not, it was, it’s proven in the US for horses. Not for, but and it it is approved in other parts of the world, obviously as an asthma medication. But yeah, in the US it, it was never approved for for treating for treatment
[01:19:39] Dr Mike T Nelson: in humans. And I think that was due to potential risk of side effects.
Correct. Which yeah. Can be debated. Yeah. Yeah. And last part too is that some of these things have permanent effects, especially in women. But the couple guys I know who, I wouldn’t say their names, but competed in the, I fv a very high level, it’s not uncommon for them to be on a replacement dose the rest of their life.
Even once they decide not to compete anymore, they’re done with their competitive days. It’s pretty common from what I’ve seen for them to. Their just own production just doesn’t recover a lot of times. So now they’re permanently on an H R T dose the rest of their life, which, the people I know, they were fine with it.
But again, something to think about that I don’t think is talked about enough in terms of the risk of people are like I’ll just go on for a little while and I’ll do this, and then I’ll go off later and I’ll be fine. That’s not always necessarily true. You’ve got acute risk and then you’ve got potentially maybe dealing with a chronic condition potentially the rest of your life
[01:20:37] Dr. Guillermo Escalante: too.
Yeah that’s a really important point because there are some potential long-term side effects, particularly, somebody that use, peds for, a month, two months, a short period of time. Probably gonna be fine after, after after a few months being off and if things will rebound fine.
But now, if you’re talking about somebody who’s been using for 5, 10, 15, 20 years on a regular basis yeah. So lot. And he actually see this, I, there there’s Dr. Thomas O’Connor actually treats a lot of individuals with this and he actually sees a lot of men who have been long-term.
And the reality for them is the, it’s not coming back. Their natural testosterone levels never come back. Doesn’t matter. You know what? Post cycle recovery therapy you use it, it just doesn’t come back. Fertility issues may be another thing that you want to consider for both men and women.
There, there are individuals who are unable or have very diffi very difficult times, having children, or if they do, they have to spend thousands and thousands of dollars in clinics to try to make that pregnancy happen and be able to have that baby. So those are things that you do want to consider which you maybe don’t think about too much when you’re, younger.
And we’re all invincible when we’re 20, at least we think we. At least I thought I
[01:21:46] Dr Mike T Nelson: was . Yeah. Yeah. And very last point, and we’ll get information on, people can contact you, a few other people. I know if you travel a lot and you go to other countries, keep in mind that even if you’re doing an H R T dose or you’re carrying a personal amount with you, make sure you check what that country considers legal and illegal.
Cuz I’ve had a couple people got in trouble, they had a prescription, they brought it with, they’re gonna be gone for, two months and it worked out okay for ’em. But they both had a pretty few hairy days and a few different countries for getting busted with, wasn’t even a huge amount.
But in that country was the legality was way different than the country.
[01:22:26] Dr. Guillermo Escalante: They came. Yeah, no, that, and that’s a really good point as well. When you’re carrying it, and like you said, even if you have a perfectly legitimate doctor prescribed order on that when you step to other countries you should be aware of what’s going on and obviously probably have a copy of all of that stuff with you so you can actually prove your case.
Otherwise you may be in, in a lot of trouble when you get to some of these countries. So some countries are more lax than others but there are some particular countries where
[01:22:53] Dr Mike T Nelson: you have to be very careful. Yeah. Awesome. Thank you so much for all of your time today. I really appreciate it.
Thank you for all your work and education and especially, publishing a lot of this information so we can get out there and we’ve got, actual data, so hopefully people can make a more. Informed choice. Cuz again, we’re not talking about, ethics aside or whatever here it’s just, I think people, if they’re going to pick whatever path it is, they should be educated about it and know as best they can, the risks and the, potential rewards for it too.
Which I think allows people to make better decisions and hopefully that’ll reduce the risk overall. Because I think just telling people like in the past, oh, AXA don’t work don’t ever do ’em. Eh, I don’t think that’s very effective. The whole say no to drugs campaign, eh, probably did more to harm, potentially use than anything else.
Versus be educated, be more. Open about it. Cuz especially younger kids, as soon as they seem like they find out you’re lying, they tend to do the opposite . Yeah,
[01:23:54] Dr. Guillermo Escalante: absolutely. Absolutely. And I’m with you a hundred percent. I’m not a judgmental person. I’d be hypocritical if I was.
But it’s one of those things, it’s know what you’re stepping into. Know your risks know the the risk to benefit ratio and take care of your body and figure out how you can do that best. Find a work with a healthcare provider or healthcare providers that can help you do that and understand that and communicate with them.
I think those are the critical things uh, to find out, don’t go blindly with these things because hey they are drugs and they are powerful. So you need to make sure that what you’re dealing with and what the potential issues that may come positive and negative that may come with them.
[01:24:30] Dr Mike T Nelson: And where can people find more about you? I know you’ve got a lot of really great stuff you put out on your Instagram channel too.
[01:24:36] Dr. Guillermo Escalante: Yeah, my Instagram is @doctorgfit. It’s spelled out so Doctor is spelled out, not just D R D O C. T o r g fit all one word. You can also find me on on Facebook. It’s Guillermo Escalante or at Dr.
G Fit. Also if you’re not part of, if you’re in the body building community and you’re not part of the NSCA, a Body building and fitness special interest group, we actually have a, I’m chair of that committee and we have a, about 2300 members in our Facebook. And we talk about everything body building related from competitions and giving feedback to other people that they want to post their stuff on to talking about new studies that come out.
Anything that’s related. To body building and fitness. We discussed that. We have a really good active group, so feel free to chime in and you just answer two or three short questions just to make sure you’re not a robot, posting some random stuff on there, . And then I’ll approve you and we’ll, we’d love to have you.
If you’re interested in learning more about the body building, more evidence-based we also developed an entire certification program through the National Academy of Sports Medicine. I was the lead subject expert matter for that particular it’s about 19 chapters long and it’s got everything related from metabolism to fat loss to cardio, to programming, to coaching, to peds supplements basically body building A through Z.
So that’s available on the N A S M. If you just look at N A S M Physique and Body Building you can actually find that program that we just launched in October. Gives you some good
[01:26:06] Dr Mike T Nelson: information there. That’s awesome. And then, do you have any room for any more grad students or you’re full up on the academic side if people are really interested in taking a deep dive down that route?
[01:26:18] Dr. Guillermo Escalante: Yeah, actually that’s a good point. So I actually, I just took a promotion to be an assistant dean oh,
[01:26:24] Dr Mike T Nelson: congratulations. I didn’t even know that. Yeah,
[01:26:26] Dr. Guillermo Escalante: that’s awesome. Actually, just, it just happened literally in, within the last few weeks. So I actually will not be teaching, but I will still be active in my research with some students.
We don’t have a graduate program at my school, but I do work with other graduate students at other programs, so I’ll be happy to I’ve served on a couple of committees so if you have anything related to body building or. Muscle hypertrophy or, anything in that area I’d be interested in at least talking to you and seeing if you need some extra help.
I’m always happy to help graduate students in achieving that. So I’ve served on a couple of grad student committees and help them with their thesis and or dissertations to, to do that and love to collaborate. So for other researchers out there as well. I do collaborate quite a bit.
I think we can get a lot done very nicely when we when we work together. And we can be more efficient with our time when we put, I always say three brains or five brains is better than one brain. So put us all together. Yeah. And we all divide the work up. You can get a lot
[01:27:19] Dr Mike T Nelson: done that way.
Awesome. Thank you so much for all of your time and all your contributions and that’s some great stuff people can check out. And thanks again. We really appreciate you coming back on here for the second time. Thank you so much.
[01:27:32] Dr. Guillermo Escalante: Thanks so much. Thanks for having me. Thank
[01:27:34] Dr Mike T Nelson: you.
[01:27:37] Dr Mike T Nelson: You’re just thank you for listening to the podcast here. Greatly appreciate it. Massive. Thank you to Dr. Escalante for coming on here. Taking a huge amount of time out of his extremely busy schedule. To share more knowledge. On this topic would highly encourage you to check out all the links below.
Especially as Instagram has got great information there, all the other things we discussed. Or you can read a lot of the papers he’s published also. Huge. Thanks to him. Super stoked to see him again at the international society of sports, nutrition conference. Which will be down in Florida. I don’t know if it’s Clearwater or where it’s at this year, but it’ll be in Florida. This coming June.
If you’re into sports nutrition, I would highly recommend you. Make the Trek down there. I will be there again. I’ll be doing a talk. I’ll release what the actual talk is on coming up. And then speaking of conferences, I will be also at the neuro sports conference. Which will be coming up here very soon in February.
I’ll be doing a talk there on a heart rate variability that will be in Deerfield beach, Florida. So we’ll put a link in the podcast there. For both ISDN ascend conference and the neural sports conference. So why not check that out? Come out. Say hi. Again, thanks to Dr. Escalante F all the time. Thank you for listening to this podcast. If you want more information, go to my website, which is Mike T nelson.com.
You can opt into the daily newsletter there, which is free. Hit reply and tell me that you listened to this podcast. And I’ll hook you up with a very cool free gift. Just for listening. Thank you so much again for listening. If you have anyone else who you believe would benefit from this information, please pass it along.
[00:00:00] Dr Mike T Nelson: Welcome back to the Flex Diet podcast. I’m your host, Dr. Mike T. Nelson. And on this podcast, we talk all about. Things to help you with better body composition performance. All in a flexible based approach in a wide variety of other topics also. Today on the podcast. We have my good buddy, Dr. Guillermo Escalante and we’re talking all about.
Professional bodybuilders. And physique athletes. What are some of the pros and cons? And why does it appear? A fair amount of them have been passing away. Unfortunately, at very young ages. Is this related to. Health parameters, pushing performance too hard. Diuretics other types of drugs and maybe even cardiovascular health.
So we dig into all of that. Today. Dr. Escalante. Has competed both in professional bodybuilding at a very high level. Is a professor out in California. And has published extensively on this topic. So he’s got the trifecta of knowledge to help us sort through all of the fact versus fiction in this area.
And again, it goes without saying. None of this is medical advice. We were just talking to him about the current published research. At the end of the day. Everyone has to track and decide for themselves. What they feel best. And if you’re listening to this in the U S. Many of the drugs we talk about.
Especially performance enhancing drugs. Are still considered illegal at the federal level. So not only are there potentially. Ethical considerations. There are legal considerations also. None of this is necessarily advice or just want to have an educated discussion about. What does the research say?
And the goal is to provide more awareness to people. If you enjoy this podcast. Check out more information from yours. Nerdy here. Go to miketnelson.com. That is the main website that everything goes through. You can hop onto the newsletter there via various methods. And send me a note saying that you listened to the podcast.
And I’ll send you a free gift. I promise there’ll be something cool. So go to Mike T nelson.com. Get on the newsletter. Send me a note there. And even if it’s just a say hi, give me some feedback. Do you like the podcast? Who do you want to see? Same thing with the daily newsletter. So as of now, I’m the only person that sponsors this podcast. So I get to do.
Whatever the heck I want. And talk to whoever I think is interesting, who has. Great information to pass along to you. So enjoy this interview with Dr. Escalante.
[00:03:25] Dr Mike T Nelson: Welcome back to the Flex Diet Podcast, and I’m here back with a guest once again. Dr. Escalante, how are you doing today, sir?
[00:03:35] Dr. Guillermo Escalante: Doing great. Today, Dr. Nelson. Thank you for inviting me. I appreciate you having me on the podcast again. It was fun last time, and I’m sure it’ll be no different
[00:03:42] Dr Mike T Nelson: this time. Yeah.
Yeah. So we’ll link to the episode. Last time, eh, some of this might overlap a little bit, but today you just published, this was a couple of weeks ago now, some super interesting data on some autopsies from professional bodybuilders. And I’m sure we’ll link to the articles in the Washington Post.
And I, I think there was a subset of an msn just talking to him about the risks with everything from fitness competitions, physique body building. And so since you’ve actually competed at a very high level in the sport, and you’ve actually written on the topic, we wanted to get you back on here since you would be the perfect person to discuss this in more
[00:04:21] Dr. Guillermo Escalante: detail.
Yeah, I appreciate it. Yeah, it’s been it’s been nice. We’ve really gotten a lot of good information out of there. And I think. One of my missions over the last few years really has been to try to make body building and fitness just a, a sport that I’ve obviously loved for the last 24 years, just to make it safer for the individuals that are practicing it and and obviously a little bit more evidence-based as much as possible.
Tho you know, along those two lines it’s been nice to be able to try to begin to play a role in that, but there’s still a steep hill to climb and I think this is a good beginning to getting
[00:04:51] Dr Mike T Nelson: on that road. So you’re saying, you mean there’s actually like bro science and other people who are scientists in the body building field
[00:05:00] Dr. Guillermo Escalante: Yeah. Yeah. Imagine that. Yeah. There there’s a lot of bro science and I always say not to knock all the bro science because, as you and I know sometimes bros actually have it right a lot of the time. A hundred percent. Yeah. And it’s a matter of, discerning the myths from the rest of it and and then figuring it out.
And really my mission has been what the NSA’s mission is just to bridge the gap between science and application specifically in this physique field because there’s just so much misinformation out there and there’s a lot of stuff that is, you know bogus.
But there’s also a lot of good information that is available that has been done for many years where, you know, some of the bro practitioners have been doing it for, decades and scientists are just now studying and applying the scientific method behind all of it and really seeing, okay, yeah, this there’s definitely some merit to some of these things and we can tweak some of these things.
And then, yeah, some of this stuff we can throw it in the trash bin because it’s really not relevant. I’ve really enjoyed playing a part in putting those pieces of the puzzle
[00:05:54] Dr Mike T Nelson: together. Yeah. This is a two part question, but, so part one would be, what were some things, do you think that the bros were actually way ahead of the science, and then the flip of that, where do you think the science is ahead of some of the bro.
[00:06:10] Dr. Guillermo Escalante: Yeah. I think some of the basic stuff I would say, like high protein intake, that they’ve been doing that for decades. I don’t know, for 40, 50, 60 years, I think bodybuilders have been consuming probably pretty close to about a gram per pound of body weight of protein, for many years.
And of course the medical community, and even some today will still say, oh, don’t take more than the R d a or too much more than the R D A and and I think there’s definitely too much protein at one end, at some point. But we, we do have to find that sweet spot where they are.
And I think. About 2.2 grams per kilogram. That kind of seems to be a pretty good, sweet spot for most physique competitors, maybe on a hyper caloric diet, maybe going slightly higher than that. So that’s one that stands out to me. I think obviously, training volume as it relates to muscle hypertrophy, that’s something that, that bodybuilders have been doing for a long time is training with adequate volume and intensity for that matter in, in regards to their training programs.
I also think some of the other components in terms of just that are not necessarily in, in the good side of things would be, how extreme do you have to be? So before it’s you think of even when I started body building, it’s our typical diet was.
Hey you need to quote unquote eat clean and you can only eat, broccoli and chicken breasts, and your next meal should be broccoli and chicken breasts. And then of course, the thin the skin you then need to eat. Tilapia only.
[00:07:27] Dr Mike T Nelson: Tilapia. Only tilapia does that. , nothing else.
Milk. Oh my god, your skin would be so thick. You’re screwed. .
[00:07:34] Dr. Guillermo Escalante: So tho those are some of the myths that we actually, you know actually see. And it’s okay, yeah, that, that’s, we can throw that by the wayside. And then I think there’s a lot of stuff that we’re still finding out, in terms of and we need to dive deeper into the science.
And then of course, there’s this stuff that we really can’t study because of medical ethics and IRBs and all of that. We’re never gonna really be able to do randomized control trials with, what’s the ideal drug intake that’s used for performance enhancement? Performance enhancement purposes.
That’s never gonna happen. We’re never gonna have evidence-based ways to do this. All we all we can do is what’s being done and study what’s being done, and then hopefully being able to decipher, good safety measures into what are better ways, more conservative ways, and what can we be looking for so that we are not putting yourself at extreme risk of any, anytime you’re doing anything to an extreme level, there are risk involved, but how can we mitigate those risks and at least be aware of what we’re stepping into.
[00:08:30] Dr Mike T Nelson: Yeah. And do you think there’s times where the science is ahead of what some of the bros are doing now? Because I know that the, I won’t name any coaches, but certain coaches have been famous for saying, what we’re doing is like 10 to 15 years ahead of the science and then in some ways that’s true.
But any thoughts on where science might be ahead or at least is hinting towards things that is not necessarily popularly done for body building in terms of training or
[00:08:59] Dr. Guillermo Escalante: nutrition. Yeah, I would say one that kind of stands to mind I was actually talking to Eric Hels about this just a couple
[00:09:06] Dr Mike T Nelson: days ago.
[00:09:06] Dr. Guillermo Escalante: Oh, nice. Today. Yeah. And we were talking the water manipulation part, right? I think there’s still a lot of ambiguity there on, is it really necessary to deplete water before, before a competition? And I’m not a big advocate of eliminating water ever but maybe titrating down a little bit, but never eliminating but still keeping, a constant flow and being very specific with the timing.
Or maybe even is that even really necessary? Can we actually just maintain that? Cuz and this comes a lot with the terminology of what’s used in the industry, where they say, Hey, you need to come in a little drier. You need to look, you need to, he’s so dry. He came imperfect.
He’s so dry. So that verbiage. Automatically associates to you to drinking less water. Or being dehydrated. And really, w what they probably really mean is they were really lean and being really lean actually creates a quote unquote dry look because there’s obviously less of a layer between the muscle and the and the skin.
Because that subcutaneous layer is now, minimal and of course you’re gonna be able to see more striations. So looking at that practice in particular, I think we’re starting to investigate it. We did a case report with Chris Baratt last year. I actually collected some data on myself for my.
My recent show in some Oh, nice. The practices. But there’s a lot of limitations in the methodology of what we’re doing to really identify it. Some of the next things we’re gonna look at is maybe looking at bio and penis spectroscopy with some base angle stuff to see if we can actually look at the raw data rather than the actual number that, that the b i s actually spits out.
Because that might be a little bit more telling. Cuz obviously when you’re, if you’re dehydrated, you’re automatically. , all of the principles that the machine thinks that you’re right, you’re in a dehydrated state. We’re not in a dehydrated state for depleting water. It, it may actually not be a a reliable number that you’re seeing when it’s says total body water or intracellular or extracellular water.
I think in that regard, I think the science may be a little bit of a head with some of that. Also things like a lot of bodybuilders maybe would carb. Carb load and sodium deplete at the same time. When it’s yeah, we need some sodium, depending, glucose strand, porters, we need sodium plays a role in your ability to carb load properly or maybe not drinking any water with the carb, bloating that, that could have some limitations as well.
So I think this is now where science has brought some light into this. It’s okay, now there is some benefit to drinking, adequate amounts of water while you’re car bloating. And there’s also some benefit to having an adequate sodium intake and electrolyte intake in general while you’re car bloating, so that you can actually absorb those carbohydrates.
So I think some of those practices, the science has actually shed a little bit of light and, it’s basic nutrition, nutritional biochemistry and metabolism when you actually see how these things are absorbed and metabolized. But applying some of those principles and studying them a little bit further has stuff I think has
[00:11:58] Dr Mike T Nelson: helped.
Yeah, and we talked a little bit about that with you on the last podcast. And then I did a podcast with a friend Michelle, welcome, where I talked about that too. And yeah, those two areas, it just feels like to me, maybe not so much with the last few years with natural competitors, but at least with enhanced competitors, it just seems like they just threw all the physiology textbooks out the window for , some odd reason.
And do you think part of that is possibly the use of diuretics? Because diuretic use will change that equation so drastically, where if you’re a natural competitor, you’re obviously not, hopefully not using any diuretics and that is just this big kind of sledgehammer that’s overriding some of the physiology is why those areas seem to be less appreciated.
[00:12:46] Dr. Guillermo Escalante: Yeah, I think that, that’s definitely a contributing factor. They they rely a lot on the pharmacology as needed. And unfortunately, they understand. And I’m not gonna say ever, there are some bright coaches that I’ve talked to that are very Oh, sure. But for the vast majority of them, really you’re really looking at individuals who have a cliff note version understanding of of how these drugs work and pharmacokinetics, pharmacodynamics of those drugs.
And at the end of the day even if you studied, chemistry and biochemistry in, in college at a decent level you’re still not a pharmacist. You’re not a pharmacologist, you’re not a physician. So you really have very limited knowledge.
And of course you can self-educate. And this is where I see, I do see some coaches that actually have, read the, the medical literature and they do understand some of these, and you can speak to them at a very high level. And to be honest, some of you even educated me in how I do, I don’t claim to know everything.
I like to always read and talk to people and understand things from everybody. But. That’s not the majority of the individuals that are out there. Unfortunately, a lot of the coaches that are out there maybe have had, success at the local level, maybe success at the national level, have done a handful of shows or maybe won a couple of shows themselves.
Maybe they’re naturally gifted themselves and then, they read the Cliff note version or the Instagram post version of it and or watch the YouTube version of it from unreliable sources. And then now they’re cookie cutting and prescribing. And I think that’s where you see these limitations.
And they know the right words to make them sound like they know everything. Yeah. But realistically, when you really try to have them explain everything in detail, they’re really missing a lot of big chunks that are very important to understand.
[00:14:25] Dr Mike T Nelson: Yeah. What I commonly see, The use of a few key terms with that doesn’t mean that they understand it.
They’re like, oh, this is a loop diuretic. And you’re like, oh, a loop di oh my God, you must know what’s going on. It’s you could have got that from Wikipedia. That doesn’t mean you know shit, . Exactly. Maybe you had some other people, sadly, but yeah, there is no guarantee that you’re gonna get it correct,
[00:14:45] Dr. Guillermo Escalante: per se.
Yeah, exactly. Exactly. Or they understand the sodium potassium pump. Okay so what, yeah. , that’s a very small part of some of this stuff, or or it’s a potassium sparing diuretic, okay, but so what does that mean in the big picture of things?
[00:15:01] Dr Mike T Nelson: Would you agree that in terms of if we’re looking at risk, That the acute risk in terms of the short term risk, that diuretics would probably be one of the more riskier things that enhanced competitors play
[00:15:14] Dr. Guillermo Escalante: with. Yeah, absolutely. And I think they’ve been almost glorified. Actually if you read some of the, some of the original textbooks on peds, the anabolic series, I don’t know what volume it’s up to.
I think I’m looking here on my shelf. I think I have. 11th edition here on there. But anyway even reading back from the very first edition or years ago, no, 20 some years ago you read diuretics are the secret to being shredded and to having that stage physique.
And that’s really not necessarily the truth. I I, not that they weren’t used, and did play a role. But that’s not, there’s a lot of danger to that. And you’re playing Russian roulette and Absolutely. I see. That’s probably the biggest contributor to to death actually.
They even anabolic steroids, they’re, you can take 400 milligrams of an anabolic on your arm or your thigh or butt, and and you’re not gonna die tomorrow. It’s a slow cumulative effect of the effects that it’s gonna have, and it affects people differently.
Not always the same way and in different dosages, but these diuretics, if you misdose them, and then you combine a lot of these things together. And when I see combined, it’s usually a combination of, yeah, I haven’t drank water for the last, two days, and I I’ve been taking these other, performance enhancement drugs that are maybe gonna be hard on the heart.
Maybe ephedra maybe clenbuterol maybe caffeine, stacking all those regularly. And then now on top of that, you’ve added this loop diuretic on top of that now you’re potentially putting your life at risk. And that, and they’re not understanding, that it’s one, one on its own is very powerful.
You combine these and that’s when you can potentially run into life-threatening problems. So for me, I think the first line of defense in terms of what can we do to. For the health and safety of athletes is basically educate people on extreme bodybuilding practices. And the number one that comes to mind is dropping water.
And, and what’s h how much water can you safely drop if you need to drop anything at all? And number two is, using these other external drugs that are prescription drugs to help facilitate that. I think that would be be the first point. If in fact if they’ve been, if they’ve had only one drug in the I F P B and the N P C.
I would vote test for diuretics. And I, and they did try to do that in the 1990s and it
[00:17:36] Dr Mike T Nelson: failed. Yeah. They did it for one year, I think, if I remember
[00:17:38] Dr. Guillermo Escalante: correctly. Yeah. And it, it didn’t work. But to me, I think that would be, that would solve a lot of the problems right off the bat is just to ban those or test for those even if it’s randomly so competitors know that Hey I can get disqualified for this.
And number two, provide education that’s not even necessary to take those measures.
[00:17:59] Dr Mike T Nelson: Yeah. I remember the first time I ever was, aware of it, I, you probably know what year it was the. The year they carried Paul, the lead off stage. It was just like, basically just completely frozen, like on death’s doorstep.
And I was like, what the hell? And at first, you’re thinking no drugs, and then you realize that, oh, they goofed up the diuretics and it’s oh man, that’s, oh, bad .
[00:18:21] Dr. Guillermo Escalante: Yeah. Yeah. Ronnie Coleman tells a story where he, he almost didn’t make it on stage. Yeah. He almost passed out from and there’s a lot of stories like that from a lot of different individuals that, that have done that.
And that was when I was working as an athletic trainer covering the events here in Summit California and Orange County and San Diego, Las Vegas for muscle contest. The number one thing that I would see was severe dehydration. And then if I would pry and ask questions, into how they got there.
I’m not gonna say all the time, but it was not infrequent for me to hear that there were some sort of prescription diuretics involved, and sometimes in very high dosages then would be indicated, for any reason. But of course you’re taking something that’s prescribed for blood pressure management or, congestive heart, Baylor management, and you’re a healthy individual and you’re taking these and you have other things going on in your system that yeah, it’s not the wisest choice.
[00:19:14] Dr Mike T Nelson: Yeah. And I’ve heard stories and rumors of people using certain drugs and forgetting that the route of administration will dramatically affect the pharmacokinetics. So if they were doing it orally versus an iv, it might be the same drug, but you’re gonna have profoundly different pharmacokinetics just by changing the route of administration
[00:19:36] Dr. Guillermo Escalante: too.
Yep. Absolutely. And then just understanding the half-life of some of these drugs, that it’s a cumulative effect. It you can’t necessarily take some of these drugs, at 6:00 AM 10:00 AM 2:00 PM 6:00 PM because hey, like that first dose is gonna be working for 12 hours, right?
. So it’s a slow continual process. And then, by the time you’ve now given two to four doses now that’s gonna be in your system for a long time. And those doses are accumulating on each other which is gonna have some potentially catastrophic
[00:20:07] Dr Mike T Nelson: effects in terms of risk management.
If someone is say, at a show and they believe someone is having any issue with diuretics. So there’s some, cuz I know you’ve worked at, several shows and seen a lot of stuff that’s happened. Is there anything in particular that someone should do because, and we’ve talked about this before, my fear is like even a lot of, e m T and very good professionals are, I don’t know if them coming upon the scene and having no idea of bodybuilding culture would think of diuretics as a potential issue just because it seems to be much more in that culture and is not something they would just run into in their normal day by day
[00:20:49] Dr. Guillermo Escalante: profession.
Yeah. I think that’s one of the biggest issues, which is why I was such an advocate of, having somebody that was in the field and even when I had this contract, I covered a majority of the events, but sometimes I would be away for vacation or I may be competing myself, and I would bring, so even though I would have another certified athletic trainer there, or even, and sometimes I would have even a another professional there.
, healthcare professional. I would actually let them know on some of the questions to ask and some of the things to look for, because you’re right, it’s not normal for a, a relatively healthy 20 some 30 year old individual to, to be taking Lasix or to be taking a, you wouldn’t even ask that question.
You wouldn’t even come to your health. Yeah. And you wouldn’t think that extreme dehydration practices are. Common unless you’re in the loop of what’s in the culture. I think of course asking the right questions is important. And asking them, for example, when was the last time you drank water?
How much water did you drink? What are you taking did you drop electrolytes or salted specifically? When, how much? When we also wanna maybe ask you might, insulin may also play a role. So maybe have you eaten carbs? Or did you take insulin? What kind of insulin, was it a slow acting, a fast acting?
What kind of insulin are you taking? So all those questions should be in there. And then you can put the pieces of the puzzle together real quick, so I know hey, okay, I haven’t had water, or I had a minimal water for the last 48. I took this diuretic and then asking what kind of diuretic they took and did they mix and match some of these?
Cuz sometimes that’s not uncommon either. They’re not just taking one, they may be combining some of these drugs root of administration is another one. And then you can put together and provide the appropriate treatment. And of course, recognizing the signs of dehydration which are a severe dehydration, which is typically, they, they’re usually not sweating much.
They have very low blood pressure. Their heartbeat is beating super fast. It’s kind of thready. They’re, they may not be with you all the time, so it’s almost like they lost consciousness, that they’re not, they may be feeling like they’re passing out, they have ringing in the ears.
So all of these things are very common. So you put all of those signs together and then you start recognizing them. And then you can intervene right away. And usually my first line of the fence is, okay well, Let’s get some fluids in you usually with some sort of electrolyte base.
So then, and then let’s get them, let’s get that in as quickly as possible. And then of course, try to get them in a comfortable position and then monitor them over time. Of course some of the athletes are very hesitant. It’s oh, I don’t wanna spill over before my show. I’m like , if you may have another show spill over, you may kill over.
So right let’s get these fluids in you right
[00:23:22] Dr Mike T Nelson: away. Yeah, no, I think that’s super useful because just in terms of, I always think of risk management, right? If more people are educated on it, hopefully there’s someone there who maybe listens to this podcast or, will know to remind, the medical professional or actually, do something there to help them.
Because correct me if I’m wrong, giving someone. Extra fluid in water isn’t gonna make anything worse, but may potentially make a huge difference in terms of risk
[00:23:51] Dr. Guillermo Escalante: to benefit ratio. Yeah, absolutely. Absolutely. Especially under those conditions. And that’s why you have to ask all those questions.
But, and if that’s gonna, you’re probably nine times outta 10 you’re gonna be right. And maybe 9.9 times outta 10, you’re gonna be right. And there’s gonna be very little detriment to providing them with any fluids at that point in time. So I think that’s important.
Absolutely.
[00:24:13] Dr Mike T Nelson: Yeah. And also I think the use of insulin is a good one too, because I did ski patrol for probably 10, 12 years. And one of the things I remember from training is if you have someone who is out skiing, snowboarding, you don’t know if they’re diabetic or not, we always used to carry like the little it’s basically like cake frosting, right?
. So it’s just a sugar you put under their tongue, depending on what if their blood glucose is too low or too high. Either way, you don’t know at that point, but if it’s too low, you could potentially save their life. If it was too high, adding that small amount of glucose is not gonna make ’em any worse.
So we just exactly did it all the time routinely, and then they would sort it out on the other end because either way you weren’t gonna make the person any worse and you potentially could. Save them in the acute
[00:24:55] Dr. Guillermo Escalante: setting. Yep, exactly right. And that’s the same thing with these fluids and regarding sugar as well.
I used to, on, in my arsenal, in my medical bag, I, I obviously had my defibrillator there. And then I also had I had some of the sugar tablets, I, Pedialyte we’re all common things that I had in there. And then I would often check, again, blood glucose levels I would check, oxygen and saturation rates, heart rate, blood pressure and then of course a asking all of the appropriate questions accordingly.
And then of course the visual inspection as I’m seeing the person and talking to
[00:25:25] Dr Mike T Nelson: them. Yeah. Cuz doing an outside medical per personnel, it almost looks like they have a hypovolemic shock. Which, yeah. Most of the time and again, this is my guess. You’re trained to think like someone, I did ski patrol.
If we see something like that and we know it’s not a glucose issue, my first thing I’m looking to see did they hit something and did they break their femur? Because if you break your femur, you could nick one of those vessels on the inside and they can just be completely bleeding out inside losing blood volume, but there’s no external bleeding or anything like that sometimes too.
So a lot of times you’re thinking like internal issue where in this scenario it could be something completely different
[00:26:05] Dr. Guillermo Escalante: too. Yep. Absolutely.
[00:26:06] Dr Mike T Nelson: Absolutely. Have you seen, again, it’s anecdotal, but in increased use of diuretics at different shows or has it plateaued or going down or what’s your, just your experience in that area?
I.
[00:26:20] Dr. Guillermo Escalante: Yeah. When I was working in the field, I would say it was fairly consistent. I would say and there were particular coaches that were known for yeah, they they’re gonna have these particular protocols and you know what those protocols are.
Those were the individuals that you had to keep an eye on. But I would say it was fairly consistent. I wouldn’t say that I saw more people using them. And sometimes some of this stuff gets recycled. You may have a year or two, or you see it less of, and then, then all of a sudden people say it’s oh you know how they used to get, shredded back in the eighties, , it was through that diuretic, and then all of a sudden you see a search.
There was actually a reason, , excuse me, posting on on Instagram where they actually posted Dorian Yates back shot, and you could see his Christmas tree in the back. And then hotty coupon’s back shot. Of course not to mention that they’re comparing different stages, different lighting, different photographers, different cameras, different angles, different positions of the pose.
Not to mention that you’re trying to compare a 2D picture to a 3D live movement, right? . So it’s not even a fair comparison of the pictures, but they were comparing the conditioning of one versus the other, and they were, the point they were trying to make as Hey, competitors in the eighties were way more shredded, way more condition, way drier than competitors of today.
So first of All those issues aside with, it’s not even a fair comparison to begin with, but all of that can add fuel to the fire because, especially if you hear the word drier, if you’re a 19 year old kid competing for your first show, I want to be dry and somebody says, Hey, let me give you some Lasix, it’s gonna really dry you out.
They’re gonna say, let’s take it, yeah. They don’t understand the repercussions of that. And then you may also have the faulty mentality of if 20 milligrams works, I wonder how much 120 milligrams works. . So then you have, a lot of issues going on with some of that.
I kind of point to say that some of these old old school types of protocols that were used, they often get recycled. And people think it’s oh, this is new. I’m like, no, it’s not new. That was done like 40 years ago. You’re just seeing it new because you haven’t been, you haven’t been alive long enough to
[00:28:28] Dr Mike T Nelson: see the cycle of it.
Yeah. Do you think some of the, I don’t know, I would say judging is quote unquote to blame because we’ve had this discussion, I’ve talked to Michelle about this too, where. I would imagine if you’re a judge, it’s easier to tell someone who’s spent, God knows how many years prepping for their show.
Maybe it’s their first show, six, eight, however many months, dieting, doing all sorts of extremely difficult things that. It’s easier to tell them you’re holding a little bit of water as opposed to you’re just not quite lean enough yet. .
[00:29:05] Dr. Guillermo Escalante: Yeah, I think that is a big problem and I think, a second line of defense into how we can make the sport safer is.
Educating judges and coaches in appropriate verbiage and terminology to use. I’ve sometimes even heard judges, some judges were probably previous competitors and some maybe may have been coaches, but not all of ’em. And sometimes you have judges who maybe don’t have a lot of background in physiology, exercise science, or even in body building, outside of being a judge giving advice on how to get the particular result.
And I think, so I think having a, providing judges a this is what your scope of practice is as a judge is basically to provide feedback and then how can we provide that feedback effectively and being careful with some of the verbiage that is used because you are right. I think sometimes judges.
To not hurt the person’s feelings, who’s been dieting for the last, four months, five months. And then you tell ’em, it’s yeah, you need to lose an extra six, eight pounds of body fat. And the person is really? Why
[00:30:04] Dr Mike T Nelson: are you crazy? What? You don’t know how much I’ve suffered.
[00:30:08] Dr. Guillermo Escalante: Yeah. And the, and that’s the reality is most people to really. Truly stage ready. At least in the in, I’m gonna talk about the men’s open division at the national level or at the professional level? Yeah, it it’s painful and it’s extreme dieting practices and it takes a long time to get there.
And when most people think when they’re ready, they probably, most of ’em could afford an extra three to six weeks of extreme practices in terms of dieting to get there, to be leaner to be competitive in the leanness component, because that’s currently what’s winning into shows is what I’m saying.
So that has a lot to do with it for sure.
[00:30:45] Dr Mike T Nelson: And how much of it related to judging too, is just the never ending push to be more extreme. Like I know they’ve, like for example, like they have a men’s classic physique now and. I don’t know if you would agree with this or not, but the first few years they had it, I’m like, oh, that almost looks slightly attainable.
Like it doesn’t look as freakish as at least the male body builders. But man, the last time I looked at the last show is I’m like, these guys look like bodybuilders 10, 12 years ago. They don’t like anything like the physique competitors or in my biased opinion of how I think it was designed to be.
It just seems like no matter what you do, everything is gonna morph towards that more extreme end of the spectrum. And I don’t know if there’s anything you can do about that other than actually changing the judging practice and not rewarding that, which is a weird double-edged sword in and of itself,
[00:31:43] Dr. Guillermo Escalante: Yeah. That, that is indeed. I think a just a a double-edged sword to say it exactly like you did because on the one end and I’m gonna, I’m gonna quote, quote Brad Schoenfeld cuz we actually talked about this when we were down in Chile. Cuz he was, Interviewed for this article in Washington News as well.
And the quote he used is, people don’t go to the zoo to see cats and dogs. People go to the zoo to see the exotic wild, the zebras and the lions and the gorillas and all of the big exotic animals, they, nobody’s interested to go see a cat and a dog at the zoo, right?
And body building is in, in the same context where people like to see the freaks in there. And that’s kinda what draws the crowd. So that being said, Because of that. It does draw the judging to be more extreme in that regard. But on the, at the same token, we also have the safety issue as to to get to this level of freakishness than more extreme practices are required.
And another analogy that I like to use is the world record in the a hundred meter dash is what, like 9.54 seconds or something like that? Yeah, that sounds about right. To see somebody run a 9.35 would be pretty awesome, but to watch somebody run a 10.05 is ah, millions of people have done that.
Yeah. So it’s the same concept where we’ve already pushed the envelope so far where, maybe changing the expectation to a more attainable state. Maybe you lose, it loses its aha moment, it loses its, it’s wow. That’s incredible.
And that’s the hard thing to balance. So it is a double-edged sword. However, I think there may be a happy medium there somewhere in between there where you don’t necessarily have to give it all up, but at the same time, you don’t have to keep pushing to those, extreme levels.
But, I just always go back cuz I was a judge for many years too. And I always think it’s but if I’m judging two competitors it’s. How are you going to judge and how do you retrain your mind to do that? Especially, so if that’s been the standard cuz we saw in women, right?
If you look at, the original Miss Olympia Rachell in the 1980s, compared to the current Miss Olympia, right? It’s a whole different look. And that evolved over time because it just, it became the norm for women to become bigger and bigger and harder and drier.
And and that kind of became the standard where, heck Rachell in the 1980s, who was Miss Olympia during her heyday, she wouldn’t even stand a chance in a figure competition, maybe not even in a bikini competition.
[00:34:05] Dr Mike T Nelson: Yeah. Yeah. And I think you even see it more profound on the women’s side, where they’ve, I think, tried to get around it by adding, more classes from body building to physique to fitness to.
Bikini. But to me as an outside observer who’s casually paying attention, it seems like the progression is still the same. If you look at the first women’s physique competitor, I don’t know when they first started that many years ago compared to now, I would be like, that looks like women’s body building 10 years ago.
It just seems like there’s this constant push towards, no matter how much they change the classes and make it, different. It seems like there’s still that drive within a, just a given period of time, because like you said, it keeps getting rewarded that you end up with something different than what I think the early intention was.
[00:34:50] Dr. Guillermo Escalante: Yeah it’s like a natural state. It’s, that’s what evolution is, right? Yeah, exactly. That , it’s like it eventually, it starts as one way and then, 10, 15 years go by or in, in evolutionary Terrance, maybe hundreds of years go by thousands of years and all of a sudden it looks completely different then.
And but that, that, that is exactly what is happening. And yeah, and I think women’s has the best analogy for that cuz even looking at bikini competitors from when they first started doing bikini to the bikini winners of today, much different figure, same thing, the figure competitors from 2000 and nine to compared to the figure competitors standing on the Olympia stage today.
Much different look.
[00:35:27] Dr Mike T Nelson: Is there anything, do you think that can be done about that? Or is that just the progression of the sport? Because like you said people wanna see freaks and all. Facets, right? I think about the, the baseball scandals with, Barry Bonds and all the stuff that happened Then, I don’t know if most fans cared because they saw more balls go over the fence.
It’s almost there’s this sort of willing part of the public to stick their head in the sand and be like, oh, I’m sure they’re all clean, but oh, they’re hitting more home runs, like drastically more. They look different, his head looks different. Oh, it can’t be anything. It’s more exciting.
We’re all good with it. But then when they find out what actually happened, everyone is paradoxically mad at the same time. .
[00:36:11] Dr. Guillermo Escalante: Yeah. And to me that’s the disturbing part is, people often wanna see the extremes of things, but they don’t necessarily wanna. What is required to get to those extremes?
They just want to see the end result. They don’t want to see the steps necessary to get there. And that requires, people call bodybuilders or even, any, anybody who’s the best at anything, they call ’em, they, if most people would call ’em, they’re obsessed with something because you are.
There is no. In being a world champion? No it’s it’s a job 24 7. And if read anybody’s story that’s ever achieved, top level of success in whatever it is, even if it, a multi-billionaire, probably unless they won, the lottery several times, chances are they’re a workaholic and they’re, that has been their life passion.
And same thing for an athlete and for a bodybuilder to, to reach the Olympia stage, that is their life. There, there is no necessarily an off button to be able to do that. And a lot of things that go behind the scenes
to
[00:37:07] Dr Mike T Nelson: get there, it seems to me like, talked about Dorian. I remember the first time, I think I saw a video of him.
Was it the Grand Prix? I can’t remember. Where, to me watching him was like, holy shit, this is like a whole. Another era. And I think part of that was the way he trained. No one saw pictures of him. There wasn’t the internet back then, like there is now. Like I think he had the ability and obviously had an incredibly freaky physique, very dry, conditioned, all that kind of stuff.
But I think the fact that he showed of showed up out of nowhere that to me it just seemed like at that point everything got much more extreme than what it was before, and it was already very extreme. I don’t know what your thoughts are on
[00:37:55] Dr. Guillermo Escalante: that. Oh no he’s definite, Lee Haney was an amazing champion.
Uh, Oh yeah. And he, and obviously he’s the whole title for most Olympics in a row. But after the Lee Hena era came, the Dorian Yates era and that’s when you see, a sharp change in in the evolution. Of body building. And then of course, after him, then came Ronnie Coleman, and then Ronnie Coleman took it to a whole new level.
Even Ronnie Coleman, when he won his first Olympia to Ronnie Coleman, when he won his last Olympia in terms of his muscularity and everything, even though, personally, my favorite Ronnie, was in that probably 99 2000 area, . But he continually got bigger and bigger and still came in, in, in condition, in good condition.
And that’s just everything was just, everybody was just chasing that, right? And I, and I love some of those physiques of the 1990s and early two thousands with, Kevin Labron and Sean Ray and gosh, just Flex Wheeler, watching some of those guys over the years was amazing to see them.
But but yeah, just looking at those people that I just mentioned, for example, lot of ’em were just so in, in such incredible shape and condition and by today’s standards, they’re actually be, they’re rather small compared to what some of the competitors are up there today.
[00:39:02] Dr Mike T Nelson: Yeah. It seems to me like there isn’t much difference from some of, at least on the male side, from some of the top physiques now. And again, I don’t follow it as much as I used to, but it seems like that just has disappeared. Like even to go back to the time of, Arnold, where you had Arnold, you had Franco, you had Zane, you had people who had very different looking physiques that all, placed well.
And then even back, like when you were talking about with everything from Frex wheeler to Ronnie, to even Jay Cutler to it, did it seem like over time they all started morphing and looking very similar? We’re now. I don’t know. They all just, maybe I’m too much of an outsider, but they all look very similar now compared to what they used to.
Maybe I’m just one of those two old school people that’s back in my day when I was watching it, type thing. .
[00:39:51] Dr. Guillermo Escalante: Yeah there’s definitely been a lot of again, like an evolution in the sport and in what we see up there and really what qualifies And then obviously what wins?
I will say this year big Romi took fifth place and he’s by far the biggest competitor there. And I think top two were Derek Lansford and and Hotty. And realistically, I think if I had to put money on it, I think they were probably on the lighter side of the competitors.
But they’re also relatively shorter, , to compare to some of those guys. They. So in terms of muscularity, they were still big, of course, but compared to Rami, he had more beef on them compared to Brandon Curry. He had more beef on them too. They just were a little bit more symmetrical, flowed a little bit less, less gaps in their physique.
And then of course they came in better condition which is, I was glad to see them win. And I thought they showed up very well in, in presenting a good package. But so yeah, so in that regard, it was a little bit different because it, it was a war rewarding big Romy and I am one of his fans.
I like him as well but his physique is very different. It’s more on the mass heavy side than it is on the other components of
[00:40:56] Dr Mike T Nelson: the judging. Yeah. And then it seems like there’s a common belief, maybe it’s not common, but that. If I took the same drugs as what these top competitors are doing, that the drugs just do all of the work for you.
And I think of the Louis Simmons quote who granted it’s power lifting, but he was from me as an outsider looking, probably one of the first guys I ever saw that was like, yeah, we use drugs. And he was very open about it. And I was like, whoa. Oh my gosh, how is that possible? And I remember someone asking him in an interview and he’s yeah, I got a gram of testosterone in the back and a denim shirt.
I haven’t seen it lift shit so far. , and his whole thing was that yes, we are using a lot of drugs, but it, the drugs aren’t doing all the work where it seems like an outside perspective would be if I was using the same magical whatever cocktails these professionals are using, then I would look the same as them.
But you go back and you look at pictures of. Ronnie Coleman, for example, his first show where he was, natural, he was crazy looking like Lee Priest when he is 18, 21 years old. You’re like, what the hell is that? Like these people were, Kai Green competed for years as a natural body, but they’re in tested divisions.
I think people don’t understand that these guys were freaks before they, did anything in terms of enhanced competi.
[00:42:19] Dr. Guillermo Escalante: Yeah, I think that’s a really good point to highlight, especially for the listeners that are on the younger side, maybe are aspiring bodybuilders because the drugs aren’t every, I’m not gonna say that the drugs are more than sprinkled on the cake, but they’re not the whole cake.
The foundation of the cake still starts, number one is who are your parents? They’re genetics. Yeah,
[00:42:36] Dr Mike T Nelson: genetics, genetics are gonna play the largest role.
[00:42:39] Dr. Guillermo Escalante: Huge. Of course you can maximize, whatever genetics you have through then proper kind of the second layer foundation, which is, appropriate eating and fueling your body appropriately.
And using appropriate training programs and methodologies to, to maximize your gains in that regard. Of course, then implementing getting in enough sleep and getting that life pattern component. All of those are so important that I think are often minimized. think.
If you’re up partying and drinking, if you’re not sleeping, if you’re inconsistently hitting the gym, if you’re not necessarily getting enough enough nutrients into your diet, micronutrients and macronutrients cuz that’s another thing. People focus so much on the macros, they forget the micros.
And it’s Hey, those are important too, guys. They play critical roles in in your body actually functioning appropriately and getting maximum results. So putting all those things together, getting enough nutrients in you, all of those are gonna be very important. So I don’t care how many drugs you take, if you’re not doing that foundation, it’s not gonna work for you.
So it really takes everything together to be able to do that. And you’re right, some of these individuals they’re already gonna be the biggest, strongest people naturally. And if we go back to the home run era it’s the same thing. Barry Bonds and Mark McGuire, all of these guys, They were amazing athletes and baseball players before they even decided to jump on the juice.
Yes. The juice basically added a little extra spice to their ability to do that, but it didn’t make them a pro baseball player. Yeah. They were of that caliber well before they got there. And that being said, sometimes individuals, we’re so different that some of these people that are so gifted already, It doesn’t take a whole lot for them to Yeah.
Get to these extra benefits. Whereas some people, it might require a whole lot and some people may have a lot of side effects, taking a little bit of stuff, and other people may be able to take a lot of stuff without a lot of side effects. So there’s a lot of inter-individual vari variability there.
And yeah, just because you take the exact same stuff that some of these pros take is not gonna g. That you’re gonna look like that. And in fact, there’s a lot of people that try and they fail very miserably because just not the equation that they’re gonna get there. Even training practices, when you see some of the training practices, some of these top bodybuilders, sometimes some of ’em don’t even train very efficiently in my No.
Or smartly, but it doesn’t matter because they’re the type of people that walk into the weight room and all of a sudden they’re swollen. They don’t even need to lift the weight. They just kinda walk in. Of course I’m being facetious there, but they could do anything and, and they would grow.
Whereas a lot of people, it takes more methodical programming to be able to do that. And we see that even in our studies, right? We see hyper responds and we see non-responders using the exact same training program or the exact same supplement that you’re providing them. And you’re gonna see people that respond very well and some that maybe even.
Respond poorly, where they actually decreased their performance doing the exact same protocol so the same’s gonna hold true with these anabolic substances.
[00:45:41] Dr Mike T Nelson: Yeah. The first time I saw that was got a C S M in 2005, 2006. Stu Phillips was there presenting on, one of the studies looking at a hypertrophy study.
And I’ve talked about this in the podcast before, but he puts up a nice scatter plot of all the data that people, I think it was like a 12 or 16 week study, I, maybe it was a little longer. Most of the people are in the middle, right? They gained a few pounds, did pretty good. There was two people who were like two standard deviations, like almost off the top of the chart.
And then there was one poor bastard who got worse . And it was super funny cause they asked what’s with these two people way at the top? And that’s what kind of responded, why they did some studies looking at acute testosterone release and growth hormone and a bunch of other stuff. But to me it was just fascinating how.
They did the same program. Granted nutrition wasn’t extremely controlled. They were told to eat the same thing, but they weren’t, living in a lab or anything like that of how you can see such dramatic, results. And a buddy of mine who worked for one of the muscle megs for years and trained with some of the top pros, and he said in his experience that, he said one of the guys was Paul DeLeT would come in and train at his gym.
And he’s I don’t think I ever saw that guy do more than 60 pounds of tricep press stones ever. And his arms were just massive , right? It just seemed like he said some of the top pers that train there. And again, this isn’t all of ’em by any means, that if they just put any tension on the muscle at all, they got a response where some other people have to do something completely different.
Maybe it’s a higher intensity, a lower volume, higher volume, whatever. I think. There’s so much variability in something like hypertrophy and then you add, like you said, drugs on top of it. There’s people who are probably hyper responds to small amount of drugs. There’s probably people who can take a shitload of stuff.
And I’ve seen some blood work on people who told me what they were taking and I’m like going, oh my God, this is, they’re gonna have an H HDL of freaking four. And it was fine. I was like, you there, you what? There’s no way. And someone else doing an H R T dose, they’re, their HDL was 11.
He was like, what the heck? , just, again, very limited case studies, but just massive amounts
[00:47:45] Dr. Guillermo Escalante: of variability. Yeah. And there’s a ton of that and I think a lot of people don’t understand that component. And not only that, but. . It’s again these these performance enhancement drugs give the person the ability to actually push harder, train harder.
Yeah. Recover faster. So it’s actually not to do less. It’s actually to be able to do more and recover faster. And and that, that’s basically what helps in the process. So if you add all of those things together, and now you have somebody that’s genetically gifted, who is doing the foundation of the diet and the training and the sleeping and the consistency and taking their time, and then you add the dietary supplements and then you add the peds on top of that, then all of a sudden you get Mr.
Olympia. That’s what you get.
[00:48:32] Dr Mike T Nelson: Yeah. And last point on this, and we’ll talk a little bit more about some of the risks is taking. Advice from genetic freaks who are maybe using and making choices you’re not making for someone who’s starting out is probably not the best direction. But that’s like the history of most especially old school muscle magazines.
I remember Lee Priest complaining that he is oh my God, like all these muscle magazines, they just want me to do another arm article. He’s I don’t really train hardly any different from my arms over the last 15 years. And you look at him and you’re like, how is that even possible to have arms like that?
Yeah. But he was a genetic freak. Obviously. He trained hard, but he didn’t use a lot of ride. He didn’t do a lot of crazy shit. But you see a picture of his arms and, to 18 year old me, I’m like, how’d he do that? ? Yeah.
[00:49:16] Dr. Guillermo Escalante: What’s your secret? what he would tell you is probably extremely disappointing.
a young kid, you’re like, you mean you just do bicep curls with the dumbbells and Yeah. Bryce cable press downs with the tri, with the tr for
[00:49:28] Dr Mike T Nelson: triceps. And you and your right is doing that twice a week. Week, yeah.
Yeah. I remember the other part too, was that a video, Jay Cutler was talking, he is yeah, straight bar bench press isn’t the best for your peck growth. And then later in the video they’re asking and what did you do? What was your history? So the interview asked a very good question, what did you do when you first started?
He’s I found dumbbells are more effective. But he is in the hike high school I was benching like 4 0 5 for reps. I’m like, what the hell, ? I’m like, yeah, that might be more effective if you’re a freak benching 4 0 5 for reps in high school already. Like a straight barbell may not be the best choice for you.
But for someone who’s listening, who, like me in high school, got squished by an empty bar, yeah. Barbell bench press would probably be pretty helpful for me. . Exactly. So you published an article looking at some of the autopsies of some bodybuilders, and it just seems in the media, maybe it’s because of the internet, maybe we have more exposure to people.
Maybe we know more about these things than we did before, but at least to me, it seems like in the last five years or so, the amount of deaths in body building in general seems to be more of a escalating, and especially people at a much. Younger age. I know Bill Pearl unfortunately just passed away recently, but it seems like the people who did it many years ago have, been able to live relatively long life where we have a lot of people who are much younger, sooner younger, appear to be passing away much sooner than in the.
[00:51:04] Dr. Guillermo Escalante: Yeah, that, that’s definitely what we noticed as well. And really what kind of caught my attention was right around 2020 2021. Dallas MCC Carver caught my attention. Yeah. Daniel Alexander caught my attention. He, he was 30 I remember he competed as a middleweight when he won the U s A championships, and I followed his career and, he died at age 30.
[00:51:24] Dr Mike T Nelson: He used was Dallas even 30. How old was he?
[00:51:26] Dr. Guillermo Escalante: He was very young. Yeah. Dallas was only 26 when he passed away. Yeah. Yeah. And then John Meadows, is 49 man and the list goes on. And of course, and there were some that died relatively young that, we actually made our cutoff at 50.
Okay. So what we specifically did is we basically just did a very generic Google search to see what, where do we, where can we find individuals who have reportedly died? Of some of any condition, first of all. And then we eventually narrowed the search down to people, body billers who had died, body billers, who had died, who were under the age of 50, between the years 2010 to 2022.
We did the search in February of 2022. And then we started narrowing and filtering down. Ultimately we, we really wanted to find the autopsy reports of these individuals. Cause we wanted to see, okay, are the re are the reported cause causes of death? Because they weren’t in medical journals necessarily.
So are these reported causes of deaths actually, The actual reported causes deaths that the coroners reported. And we started narrowing the list. Of course we had to narrow it down. We had people from all over the world, from Italy, from from great Britain who had passed away. Of course we can’t get autopsy reports for those individuals.
At least not easily. So we were able to narrow it down to people in the United States who had that. And then we actually finally started calling coroner offices. So we had a large number of individuals who had actually passed away over 40 worldwide. And then by the time we got down to the U S A, it was that were under 50 that were related to either some court, some sort of cardiac condition or an unknown condition cuz we wanted to investigate that further.
We included that in our search. And then we had about 14 that we narrowed down to for that point in time. Then we called the coroner’s office where we were able to try to get the coroner reports we’re actually able to get seven coroner reports from those individuals. So that’s basically what our analysis is based on.
Unfortunately, one of those individuals did not die of a heart related issue. It was actually a suicide. So we disregarded that. Cause our focus was on cardiovascular related events. However, it’s should be noted that there is some research to suggest that brain health and depression are an issue.
So it shouldn’t be ignored completely because that is another study in its own really is looking at the potential. Mental side effects that it may have over time, particularly when they’re coming off cycle. There is, again, very preliminary evidence to suggest that there may be some sort of link there.
Hard to identify a true cause and effect, but there is something that, that I think should be investigated further. But we focus on the cardiovascular related events. And you know what we found was there were some common threads that were in a lot of these reports. Before I go further, I wanna say there were definitely some limitations in the way the coroner reports were written.
We actually discussed that in our discussion because a lot of the coroners maybe didn’t necessarily identify these individuals as potentially using performance enhancement. So the coroner reports weren’t necessarily extremely thorough. So not all of ’em had toxicology reports. Not all of ’em did a lot of extra testing that maybe would’ve given us more information.
Couple of them were quite thorough but the majority of them were not. But we did see some common threads in what the what the report showed. We actually did an average of the hearts. All of ’em had an enlarged heart. And actually the enlarged heart was about 74% larger than the reference man.
But that’s substantial with a grain of salt because I do like to say they’re bigger. Yeah, we did re use the reference man, because that’s what’s more readily available. Ideally it would be good to compare it to other non-drug using bodybuilder. But obviously you’re not gonna be able to weigh the heart of , right?
Of living non-drug using bodybuilders. So it was an impossible ask. So as a result of that, we use the reference app because there is cardiac hypertrophy reported even with healthy non-drug using weightlifters. But nonetheless, we don’t see those guys dying necessarily. So we, that’s where we always have to of look a little further.
We also saw that the left ventricle was actually significantly larger as well as compared to, to reference men of their age. So a lot of interesting facts. And then obviously we see a lot of these common things. We see basically atherosclerosis at very common thread among all of them.
We see cardiac hypertrophy, cardiomyopathy, we see lept ventricular hypertrophy. So we see a lot of these different red flags that kind of keep appearing. Some actually had some history of where you actually see, yeah, th this person had basically low h d l high l d l. So you have this lipidemia going on in
[00:56:07] Dr Mike T Nelson: some of their So low hdl high L D L you mean?
[00:56:10] Dr. Guillermo Escalante: Yes, exactly. Yeah. So we have, so we have a bad ratio of the H D L and the L D L ratio. And we see just some common threads all the way across. So it was very interesting to actually see and at the end of the day, we basically said we can’t put a cause and effect on all of this stuff, of course, but we also can’t ignore the smoking gun and we need to investigate further into what is going on.
We actually did reference several articles in the discussions that have actually. At practices of some of these bodybuilders that are natural compared to non that have actually been using. And they’ve actually measured, of course, they’re not prescribed this stuff. They’re actually, they’re self-medicating themselves.
And then they choose to be in a study and they’re looking at, for example, what happens to to their heart, to their ventricles, et cetera which happens to the, to their blood lipids over time. And typically what you do see is again the L D L level does typically go up. H d L level does go down over time.
And then we do see again that cardiomyopathy seems to appear quite a bit with some of these individuals.
[00:57:11] Dr Mike T Nelson: And part of that related to cardiac issues, do you think that’s made worse by potential? Diuretic use. So I think of, so testosterone for example is well known to increase blood, red blood cell mass, right?
So you’ve got basically more red blood cells going around and then now you’re trying to do dehydration practice on top of it. I think of some of the cyclists from the tour of France who’ve had hematic grids that are just absolutely scary. For other reasons, they’re probably primarily using E P O and other things to drive up red blood cell mass.
So they have better endurance performance. But there’s been case studies in there and reports of, cyclists getting up at three in the morning to go exercise just because they felt like their blood was getting a little bit too thick. I know that would be something that would be harder to see on an autopsy though.
Correct. In terms of multifactorial reasons related to cardiac.
[00:58:09] Dr. Guillermo Escalante: Yeah I don’t think you wouldn’t necessarily see it but there’s definitely a lot of truth with that. And this is why one of the things we were talking about earlier was you’re absolutely right. Erythrocytosis is very common with these individuals.
And that’s because you’re gonna get, increased red blood cell production from the, a lot of these performance enhancement drugs. So now you already have, more more absolute red blood cells in there making your blood essentially a little bit thicker. And then now you dehydrate the blood plasma, which is, 70 plus percent water.
But now you deplete that, but you still have this, these thick red blood cells in there which is gonna potentially create larger problems. And this is where I see the complications, where I think people don’t put all of those things together. It’s Hey, like I’ve been, I’ve been taking these performance enhancement drugs, for the last.
Six months or six years, whatever the case may be. And then, I have a, a larger red blood cell count. Now I’m gonna basically dehydrate my body, which also includes my blood plasma, making my blood thicker. So now you actually have absolute erythrocytosis at that point in time or I’m sure relative erythrocytosis at that point in time.
So you have a lot of issues going on at that, at in there that are combined with all of those. And then you may be taking the albuterol, you may be taking the ephedra, you may be taking the caffeine and you may be depleting your electrolytes. So all of a sudden you have way many more factors that are contributing to the danger of of exposing the individual to dangerous practices.
[00:59:38] Dr Mike T Nelson: And I would, we don’t really know anything about blood pressure or history or anything on these individuals, do we? Cuz I would. Imagine if you’ve got left ventricular masses increasing. Do you think some of that is from potentially the drugs? Do you think some of it is a side effect of having high blood pressure on top of it, on top of having a higher red blood cell mass?
So just the amount of physical work the heart is doing is more than what would normally be required of it on top. Potential effects from the pharmaceuticals?
[01:00:13] Dr. Guillermo Escalante: Yeah, I think there’s, we do see a lot of hypertension in these individuals and it’s not uncommon. In fact, when we did some testing.
I have an article coming out in journalist Strength and Conditioning research, but we actually see some individuals with relatively high blood pressures at some point in time, and some of ’em are dehydrated. So that’s their blood pressure being low, which if they were not dehydrated, it would actually be higher.
And in my lab we actually, I haven’t published this paper yet, but I have data of individuals that came in at different points in their contest prep. And then we would actually measure the blood pressure and they actually answered a survey and we actually looked that out. What kind of drugs they were using.
What kind of dietary practices? Training for everything. You actually see some individuals where I would actually be testing their blood pressure and I, I would see it as elevated. So I would of course let them just rest and relax for a little bit and retest it. And retest it again. And, I would see 20 some year old guys, 30 some year old guys with hypertension.
And I’m not talking like just a little bit elevated, I’m talking. 180 or 200 over one 40, so
[01:01:19] Dr Mike T Nelson: that’s significant.
[01:01:20] Dr. Guillermo Escalante: It’s high, right? Yeah. So my next step is hey, you should go to the doctor, get this checked out because this is really high. I’ve checked it, and maybe you’re just nervous, but sure we should get this checked out.
But of course I would pry and ask them with regards to what kind of performance asthma drugs are you taking? And then you see the picture kind of forming and and yeah. And unfortunately, what I like to say I was saying this again to Eric Helms just the other day is I use the terminology look under the hood, and looking under the hood means getting regular blood work.
Not only when you’re off cycle, but also when you’re on cycle. And so if you’re getting it only once or twice a year is probably not enough. I recommend three to four times a year work with a medical professional to help you interpret that blood work and have a history of that blood work with you so you can track things over time.
Check your blood pressure regularly and regularly, even on your own, you should probably check it, at least. Couple times a month, maybe even weekly to keep a marker on what’s going on with that. And if it starts to trend upward, go see your doctor and see what’s going on with that.
Checking your blood glucose levels and making sure that those, because sometimes people are taking human growth hormone for example, and that may actually make you have hyperglycemia at that point in time. We wanna make sure that we’re monitoring your blood glucose levels that regularly.
So all those things, those are very easy preventative measures that can be done by the individual. So checking under the hood on a regular basis is something that’s not done. And if they do check under the hood, unfortunately they only check under the hood when they are off cycle, which you’re missing the whole picture because.
Things should be back to normal. At least you hope when you’re not on stuff. But if you’re on stuff nine months out of the year and you’re off stuff three months out of the year and you’re only checking it, at that six weeks after you’ve been off pings when things are back to normal or at the tail end of that three months when you, now you’re giving your body three months to come off of all the other.
But you’re on the stuff nine months out of the year. You need to look into the hood when you’re actually on everything to see how your body is responding, managing, because that’s really what your insights are starting to look like over time. And again, the issues with these drugs is it’s a dose response relationship, which is related to quantity.
Of course quality, cuz there are a lot of ’em are getting underground stuff that’s not necessarily good. And then of course, length of time o of exposure that they’re doing it. So if you’re doing super high dosages with low quality stuff for long periods of time you’re gonna, you’re gonna be in for some trouble very soon.
[01:03:48] Dr Mike T Nelson: Do you think part of it could be further impacted if you were not doing a lot of, cardiovascular training? Because in essence you’re rewarded for training for hypertrophy. Now I know obviously body billers use cardiovascular training as a way to, lose fat and burn calories, but. It again, maybe I’m skewed from looking at muscle magazines, but you don’t ever really see, top X competitor, oh look, here’s this cardiovascular routine.
If you do, it’s here’s what I do to burn fat. That it seems like cardiovascular health is not top of mind awareness, and maybe that’s because they’re not necessarily being rewarded for it. So you’re doing we know at least acutely from some studies on, weightlifting, that blood pressure can spike up pretty high during weight training, which again, doesn’t mean weight training itself is bad.
But I just think about the constant force, the left ventricle would have to create against a high pressure when you’ve got, under tension and that being compounded potentially by different pharmaceutical practice, maybe in lieu of only doing cardio before a show. I don’t know if you have any thoughts on that as.
Potential risk factor on top of
everything
[01:04:58] Dr. Guillermo Escalante: else. Yeah, no, I think there’s a lot to be said to that. I think I’m gonna, I’m gonna even go one, one slight step further and looking at these old practices of bulking to extreme levels, and then, yeah. And then cutting to extreme levels so that you have this huge shift, if you’re staying within 15 ish pounds, 20 ish pounds of your competition, body weight that’s probably about the maximum that you really need, to, to really to really succeed.
If you’re putting on and what I’m saying is if of excessive body fat, right? If you’re putting on quality muscle mass, but you’re not gonna put on 30 pounds of muscle in a year. I don’t care what you’re doing, right? No. If you’re adding, if you’re a, if you’re having a lot of a, adding a lot of body fat in that point in time, and obviously if you’re doing that, they’re typically less active.
They’re still gonna be weight training, of course, but they’re typically not gonna be doing the aerobic training. So you have this. Two things working against you and I think keeping that into per in perspective is really important in terms of keeping your body fat in check and how can I keep my body fat in check and my heart healthy?
I can actually implement some sort of aerobic training into my regular training routine, even if it’s three or four days a week at a moderate to low intensity. Just to help manage both of those things. Cardiovascular health as well as the body fat management. And of course, you don’t necessarily wanna overdo it either because then you know if you’re doing an hour of cardio, Six days a week in your off season, then where can you go when you begin your cutting, right?
Yeah. You’re gonna, you’re, if you’re gonna implement more cardio, you’re gonna be doing hours of cardio. Finding that sweet balance is really good. And to me, just a minimum dose of, maybe about hundred to 150 minutes a week of a, of aerobic exercise doesn’t have to be even high intensity, but at least getting out, doing some walking doing some lights, stair climbing bicycle riding can go a long way.
[01:06:49] Dr Mike T Nelson: Yeah. I seen in my power lifting friends who go up a couple of weight classes, as they get to the end, they’re like, yeah, the only thing that’s good is lifting weights. Everything else just sucks. And the, the handful of ones who I think have done it a more intelligent manner are watching their, their blood pressure, their blood glucose.
You, you tend to see this exponential thing where they’re good, and then. All of a sudden towards the end, everything is just going haywire. Yeah. And I’ve even seen that in friends of mine who are natural competitors for body building. Like they’re doing good, everything is good.
They’re, six weeks out from a show and like their blood chemistry is just fucked, for lack of a better word, . And they’re not even using any external compounds. It’s just the stress of trying to put your body into a state that it just doesn’t want to be in period, I think is something that people.
Forget about that is just doing it and of itself is a massive stressor on top of everything
[01:07:44] Dr. Guillermo Escalante: else. Yeah, absolutely. And that’s very common. Like you said, it’s just whether you’re a natural or not, but even things like your sleeping patterns, and everything else. They’re extremely disrupted where, it’s like two hours of sleep is like a success sometimes in when you’re, three weeks out from a show.
And it’s not because you’re not trying to sleep, it’s just because you literally can’t sleep. You’re hungry, you’re uncomfortable, you’re your body is going and maybe you’re taking other stimulants, like even natural stimulants, right? Or a legal stimulants like a caffeine, right?
You’re just constantly going. So yeah, it makes it very
[01:08:15] Dr Mike T Nelson: difficult. Yeah. Our friend Eric Helms, like the best phrase I got from him, he is, Oh, you mean body building? He’s you mean competitive starvation, ? Yeah. Yeah, absolutely. I was like, oh yeah, that’s a good one. .
[01:08:28] Dr. Guillermo Escalante: No, it is. And to get to those levels of winning physiques, it, it’s it takes a lot and you have to there’s a lot of suffering involved, that’s for sure.
And a
[01:08:36] Dr Mike T Nelson: lot of sacrifice. How much do you think just the combination of, I think of GH insulin and, anabolics to me that, and again, if you look at some of the physiques they look at in terms of, intestinal growth and, guys can’t do vacuum poses like they used to. And it just seems to me that would be a, an exponential risk because there’s no real point in physiology where all three of those are all elevated at the same time.
So now you’re just of promoting. Not even muscle growth, but just growth of all tissues almost at all costs. And like you mentioned, the cardiac system. Cause it’s enclosed in basically a small bag doesn’t have anywhere to go, so it’s gonna go inward and your thickening of the chambers are gonna get bigger and that’s gonna obviously reduce the amount of, blood flow and add more cardiac stress on
[01:09:29] Dr. Guillermo Escalante: top.
Yeah, no, absolutely. And they do all play a role in, in that. And in fact, that’s one of the goals of, of competitive body builders is hey, like what’s your IGF level? Yeah. And the higher, the better in, in terms of muscle hypertrophy or actually just hypertrophy in general, but there is, again, you walk that fine line where too high can lead to other deleterious side effects that you really don’t want.
Yeah. You may wanna run it high, but not so high where you’re having all of these other potential side effects. But how do you achieve that Is basically by exactly what you said. You put all of those variables together and then you’re able to increase that IGF one.
[01:10:08] Dr Mike T Nelson: Yeah. Last two questions as we wrap up.
In terms of, words of advice of people who are. Considering, say, enhanced body building. My, my 2 cents is the good and the bad is that it’s becoming, I think, use of drugs is to become more accepted. We can argue if that’s good or bad. I do think it is easier than ever to try to get higher quality information.
I don’t know what your thoughts are on that. My bias is everyone should be free to do what they want. And again, your, if B for example, doesn’t test for steroids, so you’re not breaking any rules in terms of the competition. Other competitions are obviously tested competitions. But my goal is that hopefully people would be more educated.
They would seek people out like yourself, read the literature and try to determine themselves, okay, here is my risk analysis ratio. And after putting thought into it, Hopefully we’ll make a more educated decision. But it also seems like there’s a never ending push for, like we said, just to see, freaks at all costs.
And I’m sure there’s people who unfortunately still go into it, rather uneducated about here’s the pros and here is the
[01:11:23] Dr. Guillermo Escalante: cons also. Yeah, I think for me, the number one thing is educate yourself appropriately do understand that there are risks associated with this. So make sure you understand fully what those are.
Read the medical literature and heck, everybody’s got access to pub nowadays, or at least Google Scholar. And maybe not all articles are accessible. There’s a lot that are free access. And you can definitely read a lot of information. And I’m talking firsthand information.
It’s not necessarily opinions of professionals in the medical field, but it’s actually people that have looked at investigations and, done studies and they’re. Just reporting the data. There’s, they’re not trying to sell a story. They’re just basically reporting data on this information.
So you can actually see, all of the potential side effects that may come, on the cardiovascular system on the liver, on the kidney, on the brain. And then of course, maybe even aesthetically, I’m thinking for women, things like, your voice deepening clitorial enlargement for men, maybe acne all of those things are gonna be things that you probably wanna consider.
Understand, which ones are gonna be reversible and which ones are not. And there are certain side effects. You reach a point of no return. And like for women specifically, once your starts, starts to deepen, that’s your new voice now, right? Those are the things that you wanna consider.
There are a lot of things like obviously for the liver, for example. Obviously if you’re taking a lot of oral compounds your liver’s gonna be more taxed than if you’re doing injectable compounds. Those are some ways in which you can do that. And obviously once you stop doing the compounds and that’s gonna decrease, you’re dyslipidemia for example, that’s something that does reverse once you come off some of those things.
But it’s one of those things where if you’re. If you’re constantly on, and that dyslipidemia stays for years and years on end, then that could potentially lead to the atherosclerosis, down the line later. So I think you should definitely be educate yourself into the true risk and the and and of course there, there are aesthetics positive effects and performance benefits.
Of course, there are benefits. That’s why people are doing them. So you need to make sure that you’re weighing that you wanna weigh in on the legal aspects, right? Because there are legal repercussions for some of this. These are illegal substances, if you’re, buying them, from underground market or whatever your source is, there may be some potential legal repercussions for that.
Work with a professional a licensed healthcare professional, work with a p. Be sincere with them and find. And if you can’t have a conversation with them openly, then find one that you can have a conversation openly with. They can probably help educate you in some of the risks associated with it if they’re in the in the know of of the industry a little bit.
And they can probably help guide you, not necessarily what to take, but maybe in how to mitigate some of those risks and how to manage your risk and how to look under the hood and follow your history on a regular basis so they can actually, guide you into, Hey, look, this is what’s, this is what this, you started this and this is the result of that.
This is what’s happening internally. So you cannot help understand that don’t try to interpret that yourself. You’re not a physician, right? That’s what doctors are for. So I think there’s a lot of those things that you can definitely do and understand and obviously don’t be a SLS bag and compete in a untested, better in a tested federation and say that you’re drug free when you’re doping up, if you’re gonna, if you’re gonna decide to cross the line and compete as an enhanced competitor, then compete in like what you said, Mike the divisions that don’t test, right?
Yeah. So that way the ethical part is not really there because. You’re an even playing ground. Everybody is basically choosing to either use or not use. So let the natural competitors be natural and compete. If you wanna compete naturally, then compete in the natural federations. If you wanna utilize, compete in the untested federations and that’s your choice.
And to me, that, that’s one thing that drives me nuts is when people claim to be drug free and they’re not. And they compete in the tested federations and try to cheat the system because at that point in time, really what’s the point? So if you wanna compete and compete with the people that are using, they compete with the people that are using the performance enhancement
[01:15:25] Dr Mike T Nelson: drugs.
Yeah. Yeah. I’ve never understood that. So you’re gonna use drugs to win in the natural competition, but you just violated the whole rules of why there’s a natural competition to begin with. It’s like I. I, I’m sure people will try to do it just to say they won whatever, but yeah, I don’t, that boggles my mind, .
[01:15:46] Dr. Guillermo Escalante: Yeah, absolutely.
[01:15:47] Dr Mike T Nelson: Absolutely. Yeah. And that’s a good part about as of right now in the US of this recording, like most of these drugs are illegal and they’re not like, I think they’re still schedule one, I think, aren’t they for the most. Schedule three.
Schedule three. Okay. Schedule three.
[01:16:02] Dr. Guillermo Escalante: Yeah. But yeah, so you, even and even if your doctor is, because they’re highly regulated if you get, if you’re, if you have a physician that’s prescribing you, testosterone for example, you have to show your identifi identification and everything.
It’s very tightly controlled with all of that. And that’s the other thing, with the t r t a lot of people confuse this thing. It’s oh, I’m just on t r t. And it’s t r t is like for a clinical diagnosis of a medical condition. If you’re loose using low dosages of testosterone to enhance your perform, You are using performance enhancement drugs.
You’re not on T R T. Somebody who’s on T R T is just basically taking enough testosterone under physician or medical supervision to get their levels to a normal healthy range, not to super physiological levels. If you’re a 25 year old kid or individual taking 200 milligrams of testosterone and you’re not on T R T, you’re a performance enhancement drugs because you’re gonna be at super physiological levels
[01:17:00] Dr Mike T Nelson: at that point in time.
Yeah. It seems like some people saying they’re on T R T is just an excuse for them to be using super physiologic levels, which I think even unfortunately makes the education and everything worse, right? Yes. Because there’s a huge difference between taking a replacement dose to be back into a normal range versus, if you’ve seen blood work on people who are taking very large doses, you are.
Not just a little bit outside the range, A lot of times you’re in a different ballpark somewhere else. in terms of that
[01:17:32] Dr. Guillermo Escalante: range. Two to three standard deviations above that range.
[01:17:36] Dr Mike T Nelson: Yeah. . Yeah, . And it’s a good part too about the legality of it and then, because a lot of ’em, if you’re obtaining it through illegal means, not only do you have the law issues, potentially ethical issues, you’ve got purity issues.
A lot of these are injectable compounds, who knows, like where you bought it from. A lot of those people, there’s not a huge incentive for them to be doing the world’s best pharmaceutical grade practice in terms of sterility, making sure what’s on the label is in there, all that kind of stuff.
Like you’re in the wild west with, whatever. Dude recommended on top of
[01:18:10] Dr. Guillermo Escalante: it. Yeah, absolutely. And also, unfortunately another thing that’s become apparent is that some of the coaches are also the drug dealers in terms of some of these things.
And there, there’s an inherent conflict of interest, right? Because if you’re making more of your money on the sale of these compounds, then you want the individual from a business perspective. I’m not saying this is the right thing to do from a purely business pers perspective, you want people to buy more, not less, right?
You’re not necessarily gonna try to give the minimal effective dose. It’s no, get as much as you can because if you’re trying to make the money, that’s what you’re trying to do. And, and there, there are those ethical boundaries there that you have to be be careful with. Yeah, it’s important.
And you, like you said you hit it on the nose, the sterility issues the purity, these compounds, they can be very compromised. And just because, The label looks nice and the it’s, it says it’s got X amount of whatever. Doesn’t mean it says, it’s pretty cheap to create an nice looking label and an nice looking vial.
It’s, it takes a little bit more knowledge to actually manufacture that in under, pharmaceutical grade compounds that are not gonna
[01:19:16] Dr Mike T Nelson: harm. Yeah. And some drugs like clenbuterol, you’re talking micrograms, not milligrams, micrograms of a drug. The last I knew of was never approved in the US
[01:19:27] Dr. Guillermo Escalante: So yeah. It was not, it was, it’s proven in the US for horses. Not for, but and it it is approved in other parts of the world, obviously as an asthma medication. But yeah, in the US it, it was never approved for for treating for treatment
[01:19:39] Dr Mike T Nelson: in humans. And I think that was due to potential risk of side effects.
Correct. Which yeah. Can be debated. Yeah. Yeah. And last part too is that some of these things have permanent effects, especially in women. But the couple guys I know who, I wouldn’t say their names, but competed in the, I fv a very high level, it’s not uncommon for them to be on a replacement dose the rest of their life.
Even once they decide not to compete anymore, they’re done with their competitive days. It’s pretty common from what I’ve seen for them to. Their just own production just doesn’t recover a lot of times. So now they’re permanently on an H R T dose the rest of their life, which, the people I know, they were fine with it.
But again, something to think about that I don’t think is talked about enough in terms of the risk of people are like I’ll just go on for a little while and I’ll do this, and then I’ll go off later and I’ll be fine. That’s not always necessarily true. You’ve got acute risk and then you’ve got potentially maybe dealing with a chronic condition potentially the rest of your life
[01:20:37] Dr. Guillermo Escalante: too.
Yeah that’s a really important point because there are some potential long-term side effects, particularly, somebody that use, peds for, a month, two months, a short period of time. Probably gonna be fine after, after after a few months being off and if things will rebound fine.
But now, if you’re talking about somebody who’s been using for 5, 10, 15, 20 years on a regular basis yeah. So lot. And he actually see this, I, there there’s Dr. Thomas O’Connor actually treats a lot of individuals with this and he actually sees a lot of men who have been long-term.
And the reality for them is the, it’s not coming back. Their natural testosterone levels never come back. Doesn’t matter. You know what? Post cycle recovery therapy you use it, it just doesn’t come back. Fertility issues may be another thing that you want to consider for both men and women.
There, there are individuals who are unable or have very diffi very difficult times, having children, or if they do, they have to spend thousands and thousands of dollars in clinics to try to make that pregnancy happen and be able to have that baby. So those are things that you do want to consider which you maybe don’t think about too much when you’re, younger.
And we’re all invincible when we’re 20, at least we think we. At least I thought I
[01:21:46] Dr Mike T Nelson: was . Yeah. Yeah. And very last point, and we’ll get information on, people can contact you, a few other people. I know if you travel a lot and you go to other countries, keep in mind that even if you’re doing an H R T dose or you’re carrying a personal amount with you, make sure you check what that country considers legal and illegal.
Cuz I’ve had a couple people got in trouble, they had a prescription, they brought it with, they’re gonna be gone for, two months and it worked out okay for ’em. But they both had a pretty few hairy days and a few different countries for getting busted with, wasn’t even a huge amount.
But in that country was the legality was way different than the country.
[01:22:26] Dr. Guillermo Escalante: They came. Yeah, no, that, and that’s a really good point as well. When you’re carrying it, and like you said, even if you have a perfectly legitimate doctor prescribed order on that when you step to other countries you should be aware of what’s going on and obviously probably have a copy of all of that stuff with you so you can actually prove your case.
Otherwise you may be in, in a lot of trouble when you get to some of these countries. So some countries are more lax than others but there are some particular countries where
[01:22:53] Dr Mike T Nelson: you have to be very careful. Yeah. Awesome. Thank you so much for all of your time today. I really appreciate it.
Thank you for all your work and education and especially, publishing a lot of this information so we can get out there and we’ve got, actual data, so hopefully people can make a more. Informed choice. Cuz again, we’re not talking about, ethics aside or whatever here it’s just, I think people, if they’re going to pick whatever path it is, they should be educated about it and know as best they can, the risks and the, potential rewards for it too.
Which I think allows people to make better decisions and hopefully that’ll reduce the risk overall. Because I think just telling people like in the past, oh, AXA don’t work don’t ever do ’em. Eh, I don’t think that’s very effective. The whole say no to drugs campaign, eh, probably did more to harm, potentially use than anything else.
Versus be educated, be more. Open about it. Cuz especially younger kids, as soon as they seem like they find out you’re lying, they tend to do the opposite . Yeah,
[01:23:54] Dr. Guillermo Escalante: absolutely. Absolutely. And I’m with you a hundred percent. I’m not a judgmental person. I’d be hypocritical if I was.
But it’s one of those things, it’s know what you’re stepping into. Know your risks know the the risk to benefit ratio and take care of your body and figure out how you can do that best. Find a work with a healthcare provider or healthcare providers that can help you do that and understand that and communicate with them.
I think those are the critical things uh, to find out, don’t go blindly with these things because hey they are drugs and they are powerful. So you need to make sure that what you’re dealing with and what the potential issues that may come positive and negative that may come with them.
[01:24:30] Dr Mike T Nelson: And where can people find more about you? I know you’ve got a lot of really great stuff you put out on your Instagram channel too.
[01:24:36] Dr. Guillermo Escalante: Yeah, my Instagram is @doctorgfit. It’s spelled out so Doctor is spelled out, not just D R D O C. T o r g fit all one word. You can also find me on on Facebook. It’s Guillermo Escalante or at Dr.
G Fit. Also if you’re not part of, if you’re in the body building community and you’re not part of the NSCA, a Body building and fitness special interest group, we actually have a, I’m chair of that committee and we have a, about 2300 members in our Facebook. And we talk about everything body building related from competitions and giving feedback to other people that they want to post their stuff on to talking about new studies that come out.
Anything that’s related. To body building and fitness. We discussed that. We have a really good active group, so feel free to chime in and you just answer two or three short questions just to make sure you’re not a robot, posting some random stuff on there, . And then I’ll approve you and we’ll, we’d love to have you.
If you’re interested in learning more about the body building, more evidence-based we also developed an entire certification program through the National Academy of Sports Medicine. I was the lead subject expert matter for that particular it’s about 19 chapters long and it’s got everything related from metabolism to fat loss to cardio, to programming, to coaching, to peds supplements basically body building A through Z.
So that’s available on the N A S M. If you just look at N A S M Physique and Body Building you can actually find that program that we just launched in October. Gives you some good
[01:26:06] Dr Mike T Nelson: information there. That’s awesome. And then, do you have any room for any more grad students or you’re full up on the academic side if people are really interested in taking a deep dive down that route?
[01:26:18] Dr. Guillermo Escalante: Yeah, actually that’s a good point. So I actually, I just took a promotion to be an assistant dean oh,
[01:26:24] Dr Mike T Nelson: congratulations. I didn’t even know that. Yeah,
[01:26:26] Dr. Guillermo Escalante: that’s awesome. Actually, just, it just happened literally in, within the last few weeks. So I actually will not be teaching, but I will still be active in my research with some students.
We don’t have a graduate program at my school, but I do work with other graduate students at other programs, so I’ll be happy to I’ve served on a couple of committees so if you have anything related to body building or. Muscle hypertrophy or, anything in that area I’d be interested in at least talking to you and seeing if you need some extra help.
I’m always happy to help graduate students in achieving that. So I’ve served on a couple of grad student committees and help them with their thesis and or dissertations to, to do that and love to collaborate. So for other researchers out there as well. I do collaborate quite a bit.
I think we can get a lot done very nicely when we when we work together. And we can be more efficient with our time when we put, I always say three brains or five brains is better than one brain. So put us all together. Yeah. And we all divide the work up. You can get a lot
[01:27:19] Dr Mike T Nelson: done that way.
Awesome. Thank you so much for all of your time and all your contributions and that’s some great stuff people can check out. And thanks again. We really appreciate you coming back on here for the second time. Thank you so much.
[01:27:32] Dr. Guillermo Escalante: Thanks so much. Thanks for having me. Thank
[01:27:34] Dr Mike T Nelson: you.
[01:27:37] Dr Mike T Nelson: You’re just thank you for listening to the podcast here. Greatly appreciate it. Massive. Thank you to Dr. Escalante for coming on here. Taking a huge amount of time out of his extremely busy schedule. To share more knowledge. On this topic would highly encourage you to check out all the links below.
Especially as Instagram has got great information there, all the other things we discussed. Or you can read a lot of the papers he’s published also. Huge. Thanks to him. Super stoked to see him again at the international society of sports, nutrition conference. Which will be down in Florida. I don’t know if it’s Clearwater or where it’s at this year, but it’ll be in Florida. This coming June.
If you’re into sports nutrition, I would highly recommend you. Make the Trek down there. I will be there again. I’ll be doing a talk. I’ll release what the actual talk is on coming up. And then speaking of conferences, I will be also at the neuro sports conference. Which will be coming up here very soon in February.
I’ll be doing a talk there on a heart rate variability that will be in Deerfield beach, Florida. So we’ll put a link in the podcast there. For both ISDN ascend conference and the neural sports conference. So why not check that out? Come out. Say hi. Again, thanks to Dr. Escalante F all the time. Thank you for listening to this podcast. If you want more information, go to my website, which is Mike T nelson.com.
You can opt into the daily newsletter there, which is free. Hit reply and tell me that you listened to this podcast. And I’ll hook you up with a very cool free gift. Just for listening. Thank you so much again for listening. If you have anyone else who you believe would benefit from this information, please pass it along.
Any review you want to drop us? It would be epic. Does really help us a lot. Get more guests, greater distribution. All that fun stuff so thank you once again and we will talk to you all very soon Soon.
mikAny review you want to drop us? It would be epic. Does really help us a lot. Get more guests, greater distribution. All that fun stuff so thank you once again and we will talk to you all very soon Soon.








{kind=link}
{kind=link}
{kind=link}
Leave A Comment